

Reshaping the Lower Face Using Injectable Fillers
- PMID: 32884187
- PMCID: PMC7458843
- DOI: 10.1055/s-0040-1716185
Reshaping the Lower Face Using Injectable Fillers
Abstract
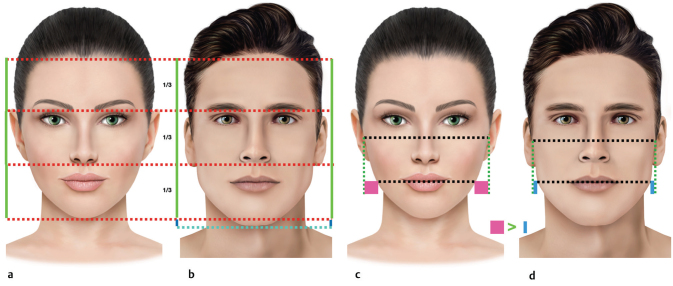
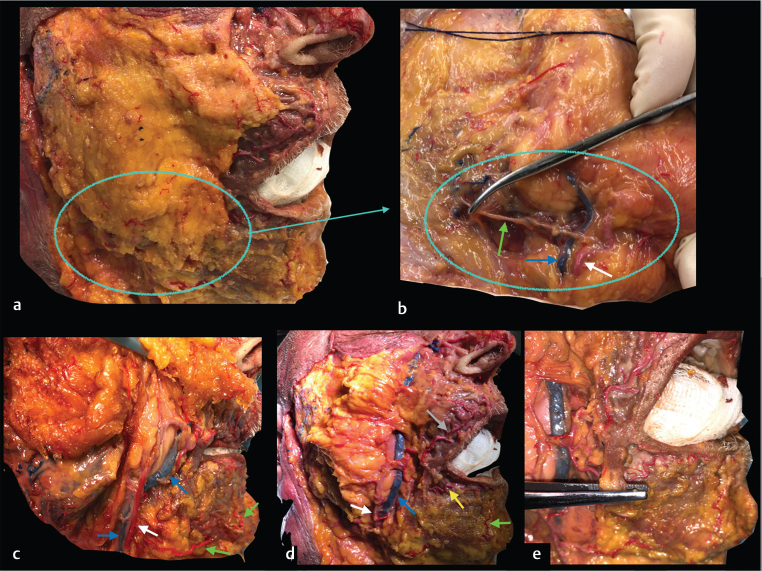
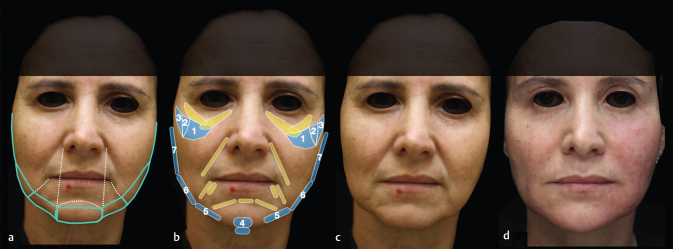
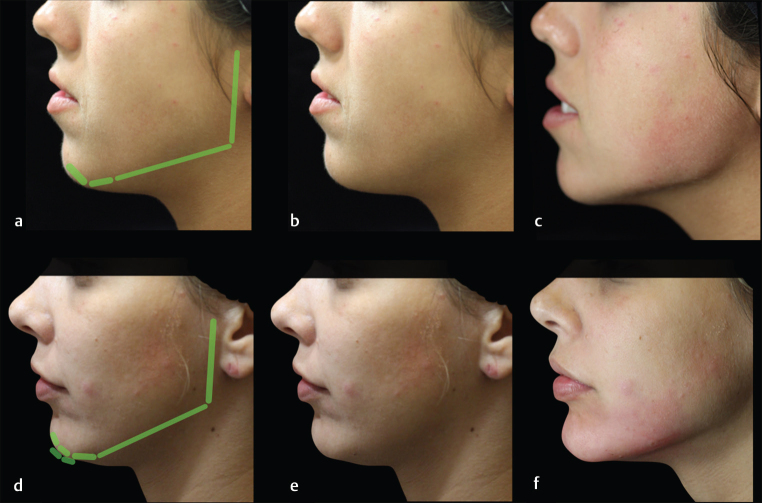
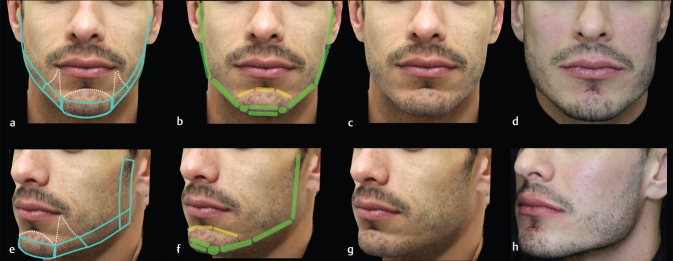
The lower third is very important for the pleasant appearance of the face. A well-contoured jawline is desirable in men and women, giving a perception of beauty and youth. It is also key to sexual dimorphism, defining masculine and feminine characteristics. The nonsurgical rejuvenation and beautification of the lower third of the face is becoming more frequent. Injectable fillers can reshape the jawline, lift soft tissues, and improve facial proportions, effectively improving the appearance of the area. It is paramount to understand the facial anatomy and perform a good facial assessment in order to propose a proper aesthetic treatment plan. The aesthetic goal of the rejuvenation approach is to redefine the mandibular angle and line. In young patients, beautification can be achieved through correction of constitutional deficit or enhancement of the contour of the face, improving the facial shape. It is very important to possess knowledge of facial anatomy and of the aging process in order to deliver effective and safe results. In this article, we discuss the anatomy of the lower third of the face, facial assessment, aging process, and treatments of the chin, prejowls and mandibular line and angle with injectable fillers. The authors' experience in the approach of this area is discussed.
Keywords: cosmetic therapies; dermal filler; facial rejuvenation; hyaluronic acid and calcium hydroxylapatite; lower face; nonsurgical.
Conflict of interest statement
Conflicts of Interest Dr. Eduardo reports personal fees from Galderma and personal fees from Underskin outside the submitted work. Dr. Braz reports personal fees from Allergan, personal fees from merz, personal fees from U.SK Under Skin, and personal fees from LÓreal outside the submitted work; in addition, Dr. Braz has a patent AB face technique pending.
Figures



References
-
- Shamban, A. The signature feature: a new concept in beauty. J Cosmet Dermatol 2019 (e-pub ahead of print). doi: https://doi.org/10.1111/jocd.12944 - PubMed
-
- Sykes J M, Fitzgerald R. Choosing the best procedure to augment the chin: is anything better than an implant? Facial Plast Surg. 2016;32(05):507–512. - PubMed
-
- Sands N B, Adamson P A. Global facial beauty: approaching a unified aesthetic ideal. Facial Plast Surg. 2014;30(02):93–100. - PubMed
-
- Goodman G J. The oval female facial shape- a study in beauty. Dermatol Surg. 2015;41(12):1375–1383. - PubMed
-
- Vazirnia A, Braz A, Fabi S G. Nonsurgical jawline rejuvenation using injectable fillers. J Cosmet Dermatol. 2019;00:1–8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources