

Access to intensive care in 14 European countries: a spatial analysis of intensive care need and capacity in the light of COVID-19
- PMID: 32886208
- PMCID: PMC7472675
- DOI: 10.1007/s00134-020-06229-6
Access to intensive care in 14 European countries: a spatial analysis of intensive care need and capacity in the light of COVID-19
Abstract
Purpose: The coronavirus disease 2019 (COVID-19) poses major challenges to health-care systems worldwide. This pandemic demonstrates the importance of timely access to intensive care and, therefore, this study aims to explore the accessibility of intensive care beds in 14 European countries and its impact on the COVID-19 case fatality ratio (CFR).
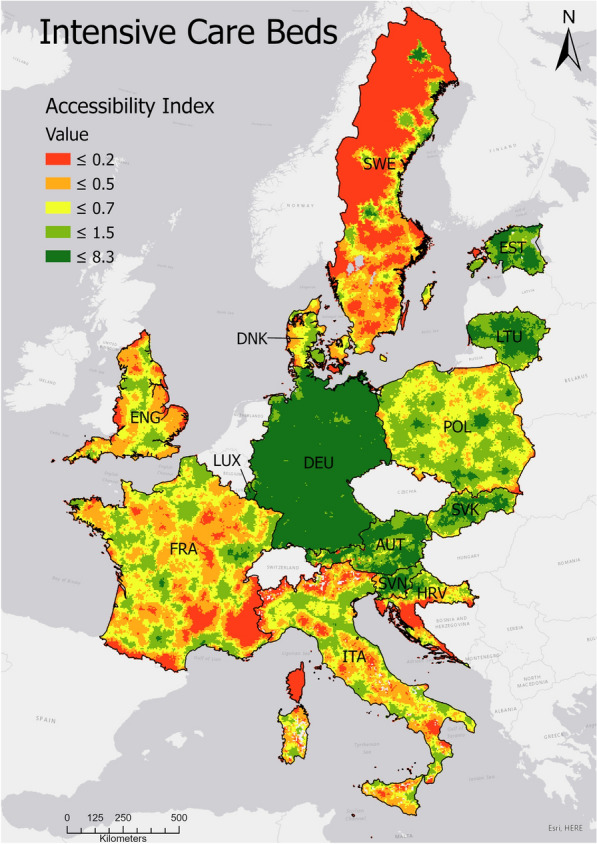
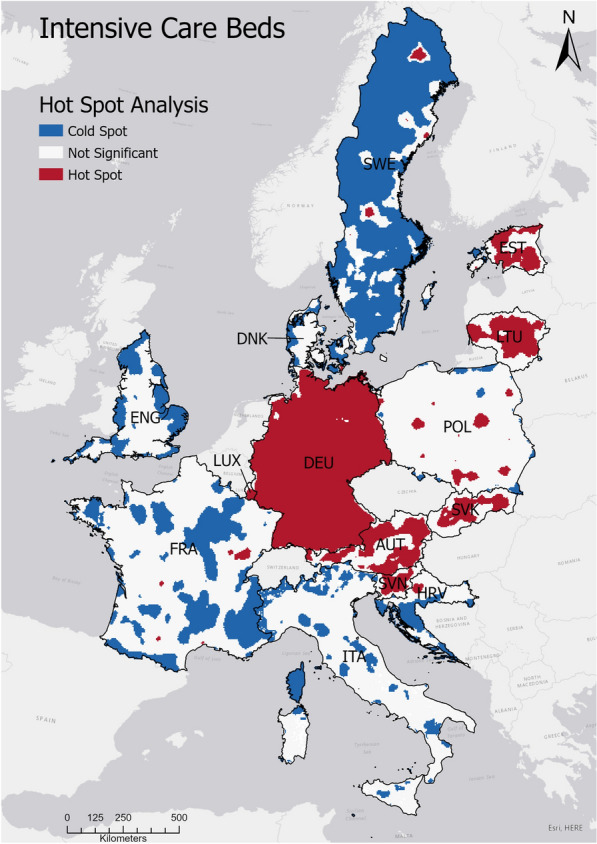
Methods: We examined access to intensive care beds by deriving (1) a regional ratio of intensive care beds to 100,000 population capita (accessibility index, AI) and (2) the distance to the closest intensive care unit. The cross-sectional analysis was performed at a 5-by-5 km spatial resolution and results were summarized nationally for 14 European countries. The relationship between AI and CFR was analyzed at the regional level.
Results: We found national-level differences in the levels of access to intensive care beds. The AI was highest in Germany (AI = 35.3), followed by Estonia (AI = 33.5) and Austria (AI = 26.4), and lowest in Sweden (AI = 5) and Denmark (AI = 6.4). The average travel distance to the closest hospital was highest in Croatia (25.3 min by car) and lowest in Luxembourg (9.1 min). Subnational results illustrate that capacity was associated with population density and national-level inventories. The correlation analysis revealed a negative correlation of ICU accessibility and COVID-19 CFR (r = - 0.57; p < 0.001).
Conclusion: Geographical access to intensive care beds varies significantly across European countries and low ICU accessibility was associated with a higher proportion of COVID-19 deaths to cases (CFR). Important differences in access are due to the sizes of national resource inventories and the distribution of health-care facilities relative to the human population. Our findings provide a resource for officials planning public health responses beyond the current COVID-19 pandemic, such as identifying potential locations suitable for temporary facilities or establishing logistical plans for moving severely ill patients to facilities with available beds.
Keywords: Access; COVID-19; Europe; Intensive care.
Conflict of interest statement
The authors state that there are no conflicts of interest.
Figures
Comment in
-
Intensive care accessibility and outcomes in pandemics.Intensive Care Med. 2020 Nov;46(11):2064-2066. doi: 10.1007/s00134-020-06264-3. Epub 2020 Oct 14. Intensive Care Med. 2020. PMID: 33052422 Free PMC article. No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
