

A multivariate model of time to conversion from mild cognitive impairment to Alzheimer's disease
- PMID: 32886293
- PMCID: PMC7732920
- DOI: 10.1007/s11357-020-00260-7
A multivariate model of time to conversion from mild cognitive impairment to Alzheimer's disease
Abstract
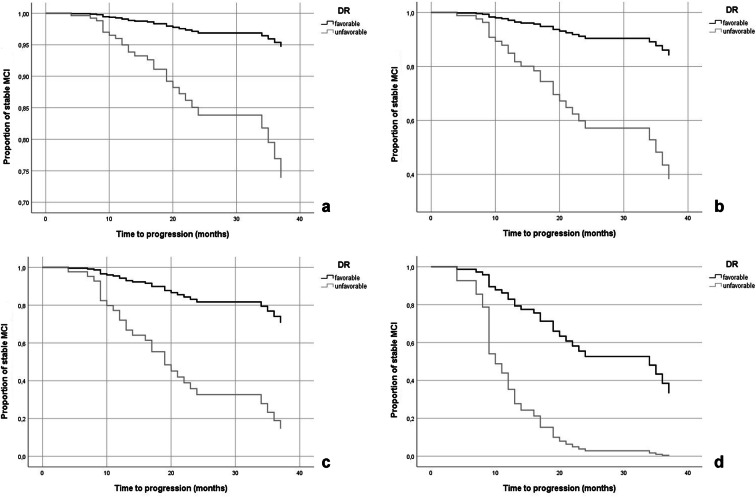
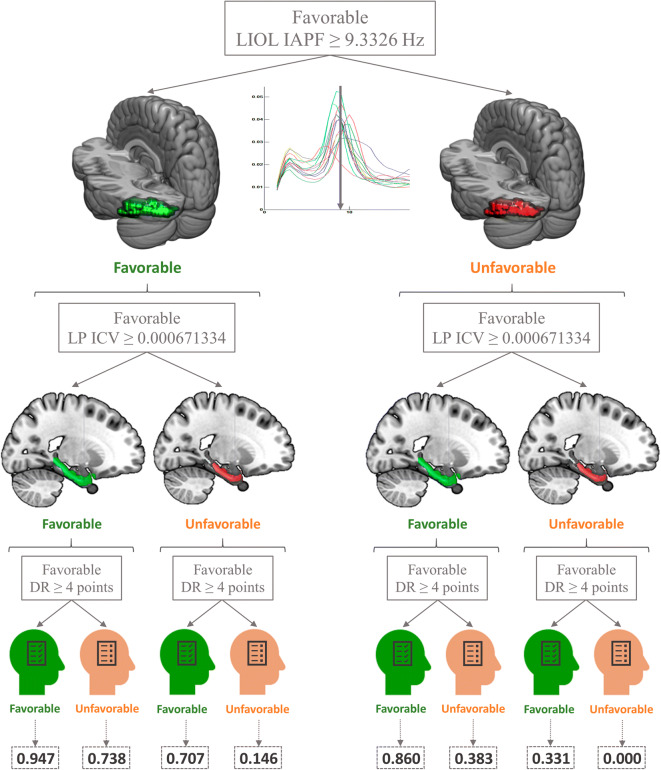
The present study was aimed at determining which combination of demographic, genetic, cognitive, neurophysiological, and neuroanatomical factors may predict differences in time to progression from mild cognitive impairment (MCI) to Alzheimer's disease (AD). To this end, a sample of 121 MCIs was followed up during a 5-year period. According to their clinical outcome, MCIs were divided into two subgroups: (i) the "progressive" MCI group (n = 46; mean time to progression 17 ± 9.73 months) and (ii) the "stable" MCI group (n = 75; mean time of follow-up 31.37 ± 14.58 months). Kaplan-Meier survival analyses were applied to explore each variable's relationship with the progression to AD. Once potential predictors were detected, Cox regression analyses were utilized to calculate a parsimonious model to estimate differences in time to progression. The final model included three variables (in order of relevance): left parahippocampal volume (corrected by intracranial volume, LP_ ICV), delayed recall (DR), and left inferior occipital lobe individual alpha peak frequency (LIOL_IAPF). Those MCIs with LP_ICV volume, DR score, and LIOL_IAPF value lower than the defined cutoff had 6 times, 5.5 times, and 3 times higher risk of progression to AD, respectively. Besides, when the categories of the three variables were "unfavorable" (i.e., values below the cutoff), 100% of cases progressed to AD at the end of follow-up. Our results highlighted the relevance of neurophysiological markers as predictors of conversion (LIOL_IAPF) and the importance of multivariate models that combine markers of different nature to predict time to progression from MCI to dementia.
Keywords: Alzheimer’s disease; Delayed recall; Episodic memory; Individual alpha peak frequency; Medial–temporal volume; Mild cognitive impairment; Time to progression.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Ahmed S, Mitchell J, Arnold R, Nestor PJ, Hodges JR. Predicting rapid clinical progression in amnestic mild cognitive impairment. Dement Geriatr Cogn Disord. 2008;25:170–177. 10.1159/000113014 - PubMed
-
- Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A, Holtzman DM, Jagust WJ, Petersen RC, Snyder PJ, Carrillo MC, Thies B, Phelps CH. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer Dement. 2011;7(3):270–279. doi: 10.1016/j.jalz.2011.03.008. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
