

Long-term risk of dementia following hospitalization due to physical diseases: A multicohort study
- PMID: 32886434
- PMCID: PMC7754402
- DOI: 10.1002/alz.12167
Long-term risk of dementia following hospitalization due to physical diseases: A multicohort study
Abstract
Introduction: Conventional risk factors targeted by prevention (e.g., low education, smoking, and obesity) are associated with a 1.2- to 2-fold increased risk of dementia. It is unclear whether having a physical disease is an equally important risk factor for dementia.
Methods: In this exploratory multicohort study of 283,414 community-dwelling participants, we examined 22 common hospital-treated physical diseases as risk factors for dementia.
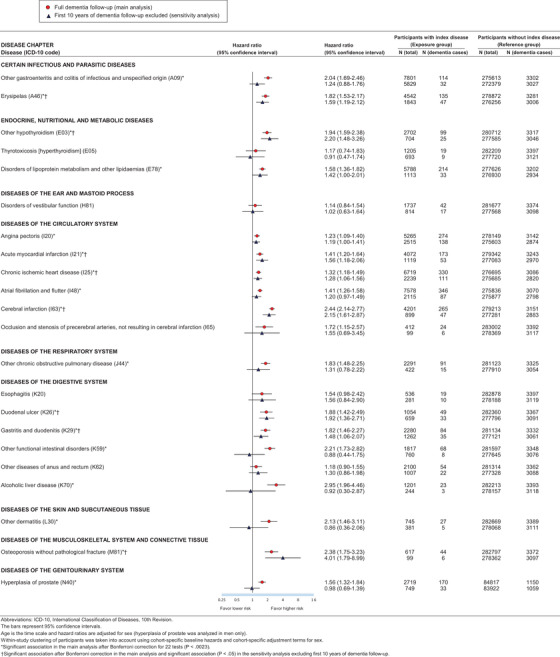
Results: During a median follow-up of 19 years, a total of 3416 participants developed dementia. Those who had erysipelas (hazard ratio = 1.82; 95% confidence interval = 1.53 to 2.17), hypothyroidism (1.94; 1.59 to 2.38), myocardial infarction (1.41; 1.20 to 1.64), ischemic heart disease (1.32; 1.18 to 1.49), cerebral infarction (2.44; 2.14 to 2.77), duodenal ulcers (1.88; 1.42 to 2.49), gastritis and duodenitis (1.82; 1.46 to 2.27), or osteoporosis (2.38; 1.75 to 3.23) were at a significantly increased risk of dementia. These associations were not explained by conventional risk factors or reverse causation.
Discussion: In addition to conventional risk factors, several physical diseases may increase the long-term risk of dementia.
Keywords: cohort studies; dementia; disease; hospitalization; risk factors.
© 2020 The Authors. Alzheimer's & Dementia published by Wiley Periodicals, Inc. on behalf of Alzheimer's Association.
Figures


References
-
- Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390:2673‐2734. - PubMed
-
- Knopman DS. Lowering of amyloid‐beta by β‐secretase inhibitors ‐ some informative failures. N Engl J Med. 2019;380:1476‐1478. - PubMed
-
- National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division, Board on Health Sciences Policy, Committee on Preventing Dementia and Cognitive Impairment. Preventing Cognitive Decline and Dementia: A Way Forward. Washington (DC): National Academies Press (US); 2017.
-
- Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines. Geneva: World Health Organization; 2019. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
