

Chest computed tomography (CT) findings and semiquantitative scoring of 60 patients with coronavirus disease 2019 (COVID-19): A retrospective imaging analysis combining anatomy and pathology
- PMID: 32886711
- PMCID: PMC7473568
- DOI: 10.1371/journal.pone.0238760
Chest computed tomography (CT) findings and semiquantitative scoring of 60 patients with coronavirus disease 2019 (COVID-19): A retrospective imaging analysis combining anatomy and pathology
Abstract
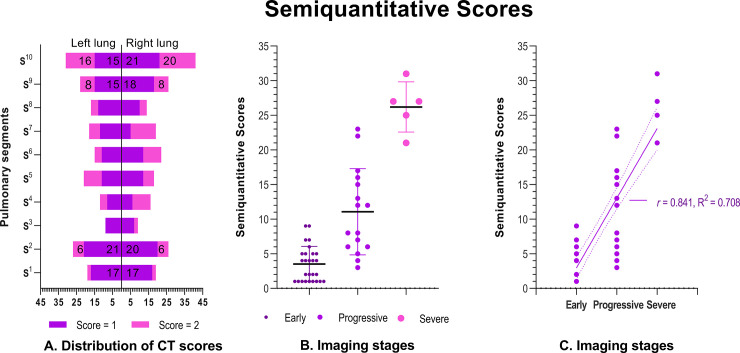
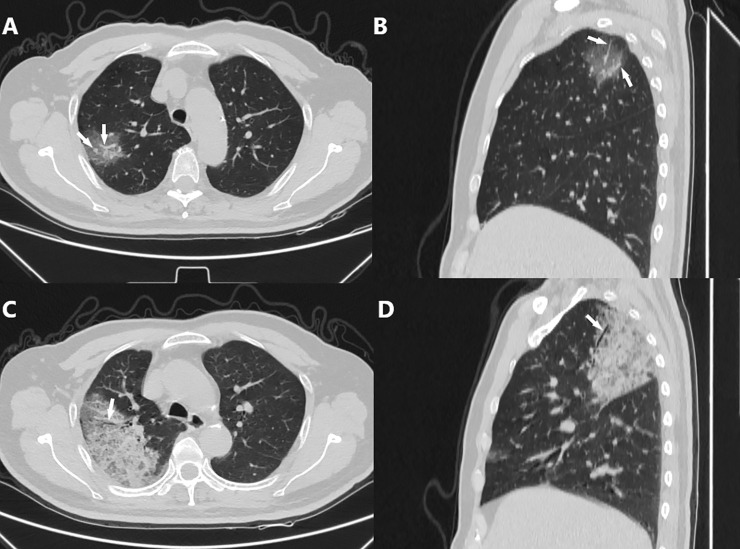
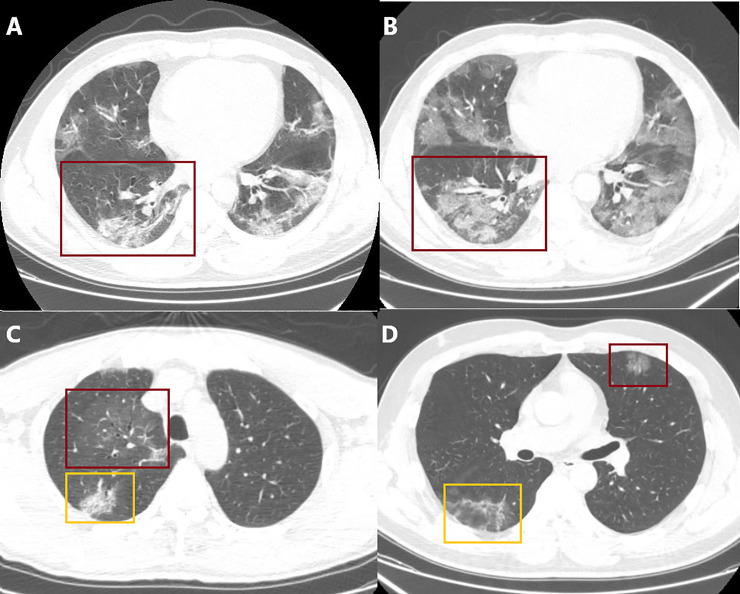
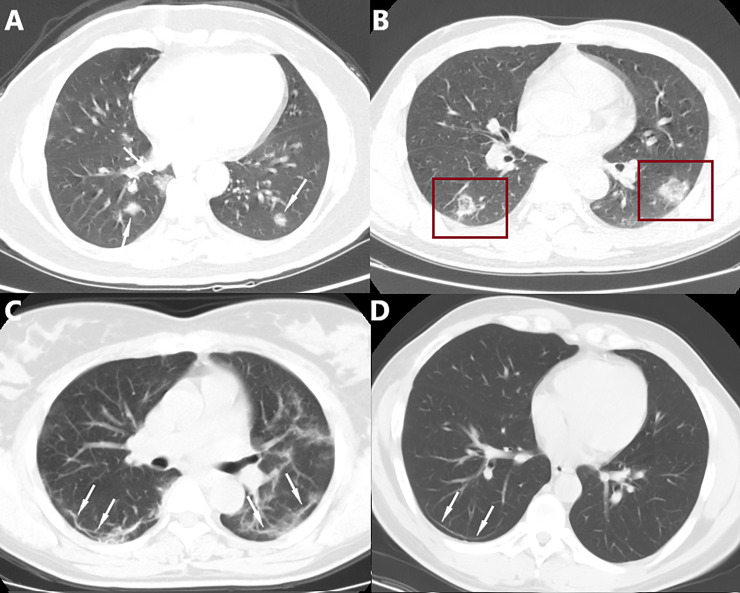
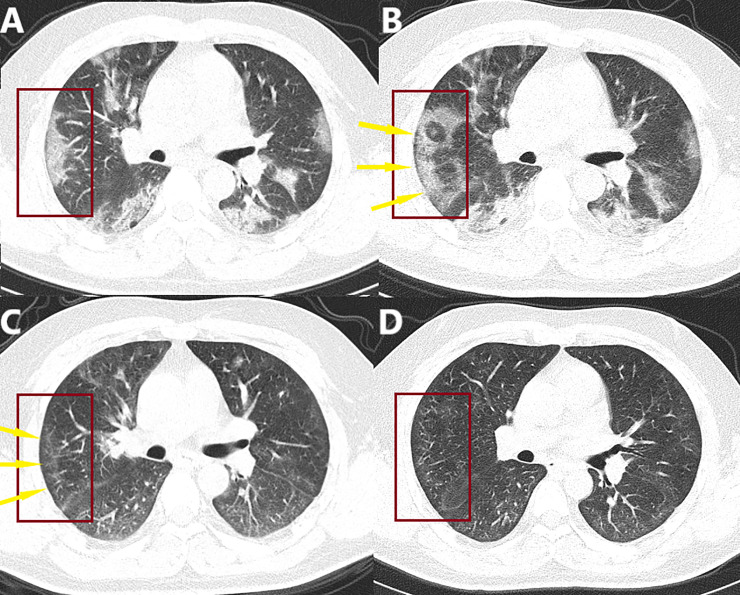
In this study, we ascertained the chest CT data of 60 patients admitted to 3 hospitals in Chongqing with confirmed COVID-19. We conducted anatomical and pathological analyses to elucidate the possible reasons for the distribution, morphology, and characteristics of COVID-19 in chest CT. We also shared a semiquantitative scoring of affected lung segments, which was recommended by our local medical association. This scoring system was applied to quantify the severity of the disease. The most frequent imaging findings of COVID-19 were subpleural ground glass opacities and consolidation; there was a significant difference in semiquantitative scores between the early, progressive, and severe stages of the disease. We conclude that the chest CT findings of COVID-19 showed certain characteristics because of the anatomical features of the human body and pathological changes caused by the virus. Therefore, chest CT is a valuable tool for facilitating the diagnosis of COVID-19 and semiquantitative scoring of affected lung segments may further elucidate diagnosis and assessment of disease severity. This will assist healthcare workers in diagnosing COVID-19 and assessing disease severity, facilitate the selection of appropriate treatment options, which is important for reducing the spread of the virus, saving lives, and controlling the pandemic.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

Similar articles
-
The role of a chest computed tomography severity score in coronavirus disease 2019 pneumonia.Medicine (Baltimore). 2020 Oct 16;99(42):e22433. doi: 10.1097/MD.0000000000022433. Medicine (Baltimore). 2020. PMID: 33080676 Free PMC article.
-
CT image of novel coronavirus pneumonia: a case report.Jpn J Radiol. 2020 May;38(5):407-408. doi: 10.1007/s11604-020-00945-1. Epub 2020 Mar 18. Jpn J Radiol. 2020. PMID: 32189175 Free PMC article.
-
A retrospective study of the initial chest CT imaging findings in 50 COVID-19 patients stratified by gender and age.J Xray Sci Technol. 2020;28(5):875-884. doi: 10.3233/XST-200709. J Xray Sci Technol. 2020. PMID: 32804112 Free PMC article.
-
CT in coronavirus disease 2019 (COVID-19): a systematic review of chest CT findings in 4410 adult patients.Eur Radiol. 2020 Nov;30(11):6129-6138. doi: 10.1007/s00330-020-06975-7. Epub 2020 May 30. Eur Radiol. 2020. PMID: 32474632 Free PMC article.
-
CT Manifestations and Clinical Characteristics of 1115 Patients with Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-analysis.Acad Radiol. 2020 Jul;27(7):910-921. doi: 10.1016/j.acra.2020.04.033. Epub 2020 May 5. Acad Radiol. 2020. PMID: 32505599 Free PMC article.
Cited by
-
Predicting malignant potential of solitary pulmonary nodules in patients with COVID-19 infection: a comprehensive analysis of CT imaging and tumor markers.BMC Infect Dis. 2024 Sep 27;24(1):1050. doi: 10.1186/s12879-024-09952-3. BMC Infect Dis. 2024. PMID: 39333962 Free PMC article.
-
Association of chest computed tomography severity score at ICU admission and respiratory outcomes in critically ill COVID-19 patients.PLoS One. 2024 May 2;19(5):e0299390. doi: 10.1371/journal.pone.0299390. eCollection 2024. PLoS One. 2024. PMID: 38696477 Free PMC article.
References
-
- WHO. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... (Accessed June 30. 2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
