

Postoperative Telephone-Based Questionnaire on Quality of Life after Robotic-Assisted Laparoscopic Hysterectomy versus Conventional Total Laparoscopic Hysterectomy
- PMID: 32887523
- PMCID: PMC7565397
- DOI: 10.3390/jcm9092849
Postoperative Telephone-Based Questionnaire on Quality of Life after Robotic-Assisted Laparoscopic Hysterectomy versus Conventional Total Laparoscopic Hysterectomy
Abstract
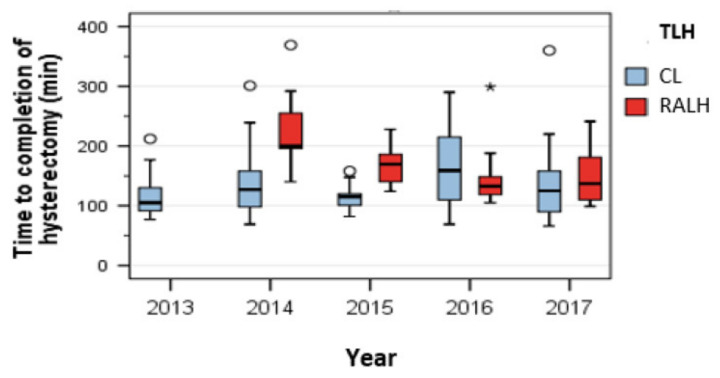
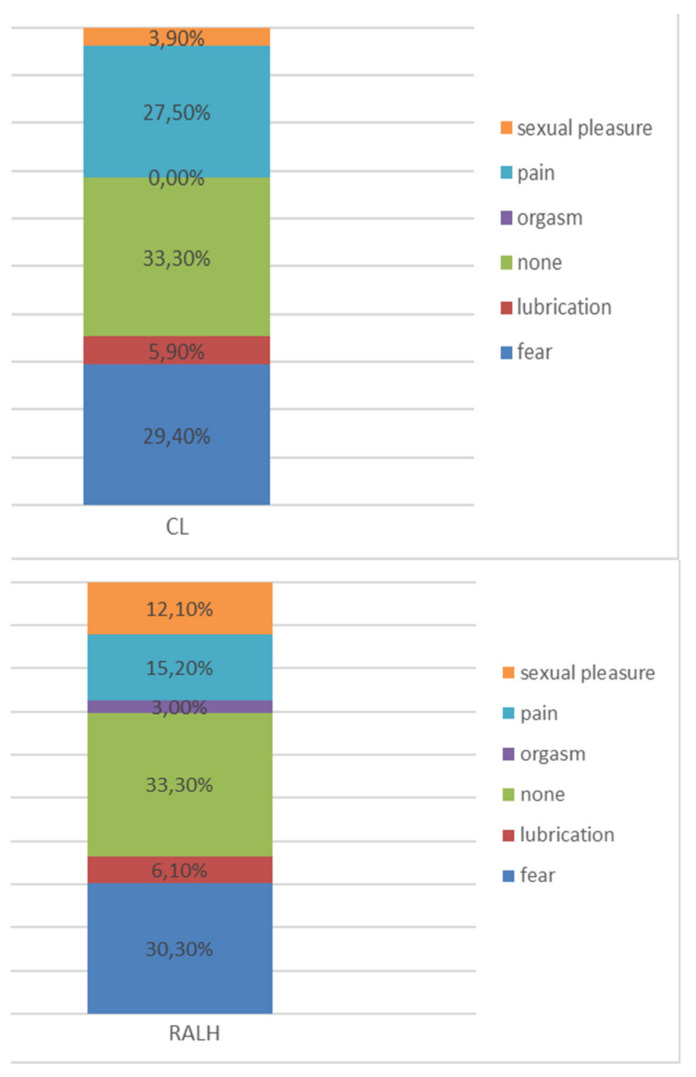
Aim: The objective of the study was to evaluate the benefits of robotic-surgery for hysterectomy compared to conventional laparoscopy for benign indications. A specially prepared telephone-based questionnaire was used postoperatively. Method: All women (n = 155) undergoing total laparoscopic hysterectomy for benign indications either by the robotic-assisted procedure (RALH) or conventional laparoscopy (CL) between 1 January 2013 and 31 December 2017 at the Department of the Gynecology, University Hospitals, Campus Kiel, Germany, were eligible for analysis. Intra-operative and postoperative parameters affecting the patients' quality of life were assessed by a telephone-based questionnaire. The latter addressed postoperative pain, limitations of basic hygiene, daily activity, active pursuit of hobbies, sexual intercourse, and days of sick leave. All patients received the questionnaire by post at least three weeks prior to being contacted on the phone. Results: 78% of the contacted patients responded to the questionnaire; 96% (n = 115) of the patients said they would recommend the operation to other patients. Both groups needed 42 days to resume their regular hobbies. In whole 90.8% (n = 108) were total satisfied with the cosmetic result of the abdominal incision; the numbers in the respective groups were 80% (80% n = 36) in RALH and 97.3% (n = 72) in CL. The difference was significant on the Chi-square test (p = 0.002). 5% (n = 7) were dissatisfied with the scar (13.3%; n = 6) in the RALH group, and 1.4% (n = 1) in CL. In all 1.7 % of patients were dissatisfied with the position of the incisions; the respective numbers were 4.4 % (n = 2) in the RALH group and no patient in the CL group. 33% of patients experienced no limitations in regard of sexual intercourse after the operation. The median number of days taken to resume sexual intercourse after the operation was 56 days in the CL group, and 49 days in the RALH group. Nearly 30% (n = 25) were hesitant to resume intercourse. The median operating time was 145 min in the RALH group, which was significantly longer than the 117 min taken in the CL group (p < 0.001). Conclusions: The RALH procedure was associated with some minor advantages for the patients according to the results, however it does not have major significant advantages, especially in regard of early restoration of sexual function, while the CL shows shorter operating times and similar limitation. Postoperative counseling of patients should be aligned to their fears and expectations in regard of sexual function.
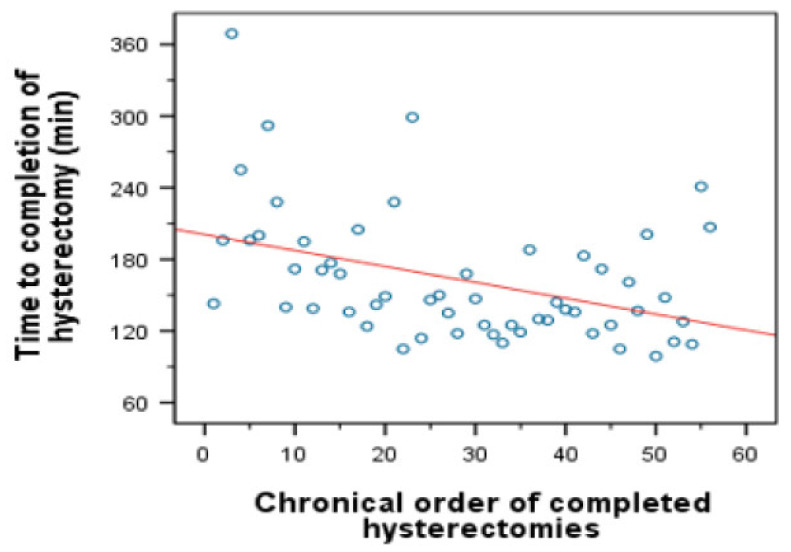
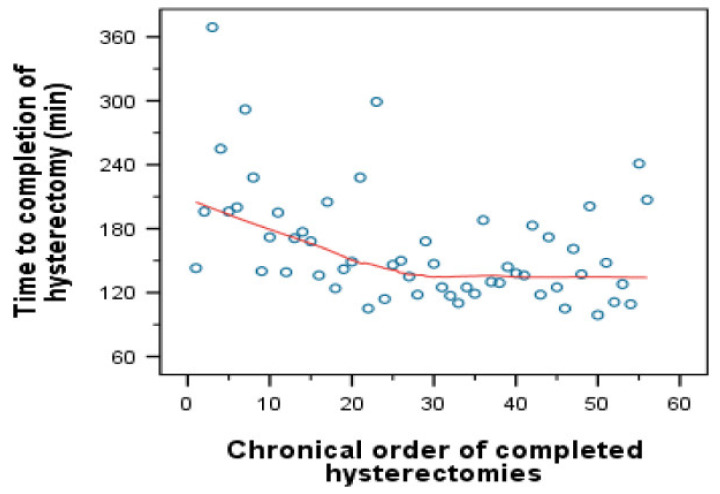
Keywords: counseling; laparoscopic hysterectomy; learning curve; patient-doctor-relationship; quality of life; robotic surgery; sexuality.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
