

Implementation and evaluation of nonclinical interventions for appropriate use of cesarean section in low- and middle-income countries: protocol for a multisite hybrid effectiveness-implementation type III trial
- PMID: 32887669
- PMCID: PMC7650262
- DOI: 10.1186/s13012-020-01029-4
Implementation and evaluation of nonclinical interventions for appropriate use of cesarean section in low- and middle-income countries: protocol for a multisite hybrid effectiveness-implementation type III trial
Abstract
Background: While cesarean sections (CSs) are a life-saving intervention, an increasing number are performed without medical reasons in low- and middle-income countries (LMICs). Unnecessary CS diverts scarce resources and thereby reduces access to healthcare for women in need. Argentina, Burkina Faso, Thailand, and Vietnam are committed to reducing unnecessary CS, but many individual and organizational factors in healthcare facilities obstruct this aim. Nonclinical interventions can overcome these barriers by helping providers improve their practices and supporting women's decision-making regarding childbirth. Existing evidence has shown only a modest effect of single interventions on reducing CS rates, arguably because of the failure to design multifaceted interventions effectively tailored to the context. The aim of this study is to design, adapt, and test a multifaceted intervention for the appropriate use of CS in Argentina, Burkina Faso, Thailand, and Vietnam.
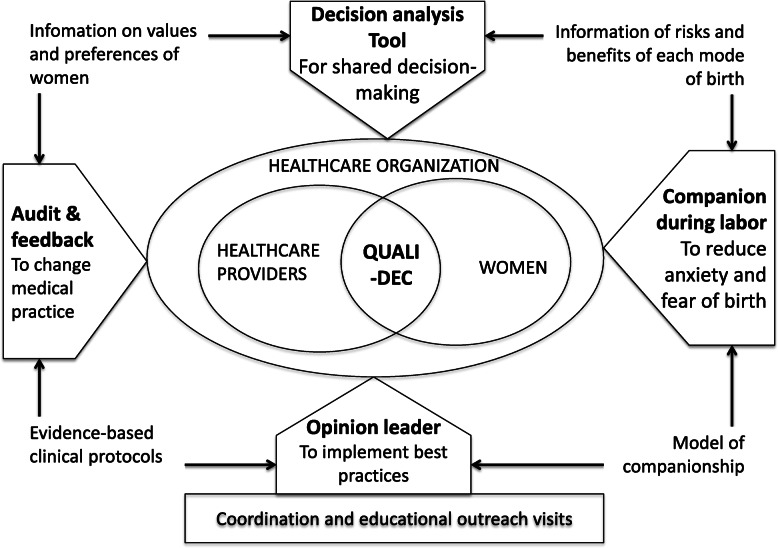
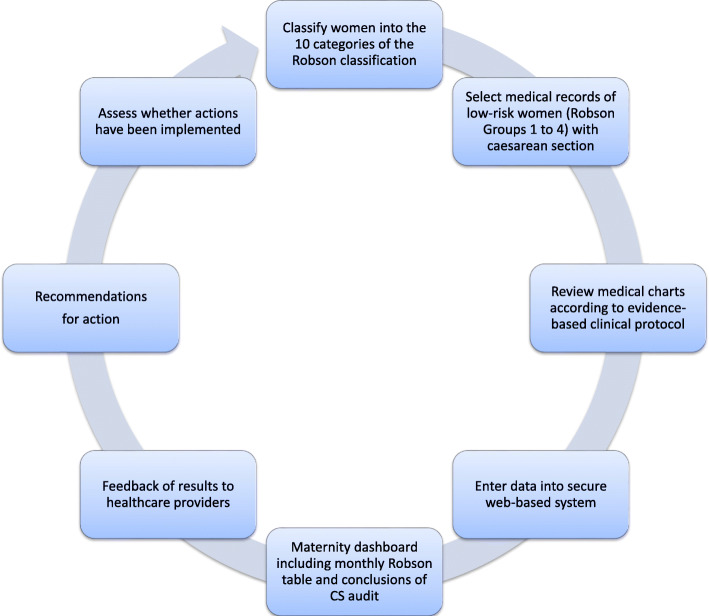
Methods: We designed an intervention (QUALIty DECision-making-QUALI-DEC) with four components: (1) opinion leaders at heathcare facilities to improve adherence to best practices among clinicians, (2) CS audits and feedback to help providers identify potentially avoidable CS, (3) a decision analysis tool to help women make an informed decision on the mode of birth, and (4) companionship to support women during labor. QUALI-DEC will be implemented and evaluated in 32 hospitals (8 sites per country) using a pragmatic hybrid effectiveness-implementation design to test our implementation strategy, and information regarding its impact on relevant maternal and perinatal outcomes will be gathered. The implementation strategy will involve the participation of women, healthcare professionals, and organizations and account for the local environment, needs, resources, and social factors in each country.
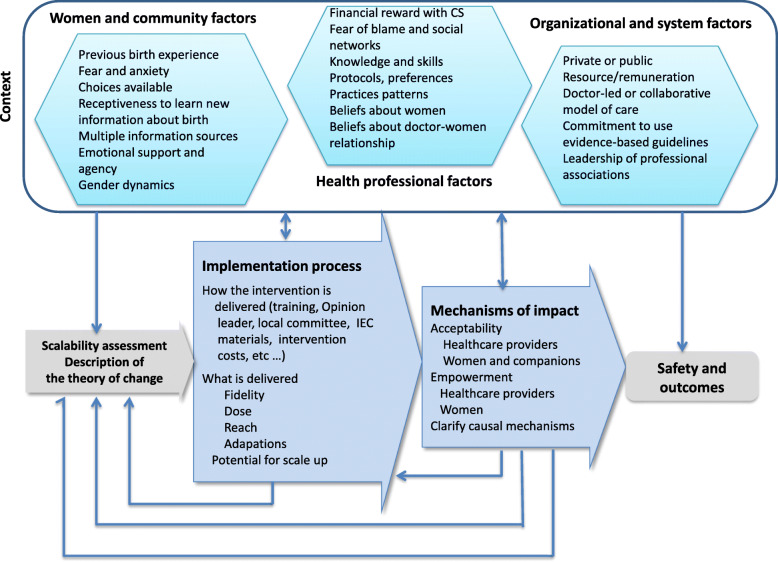
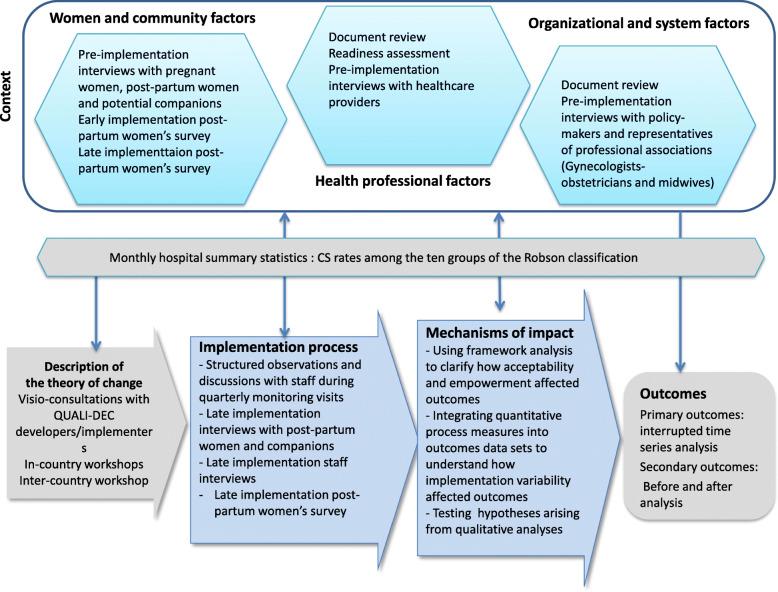
Discussion: There is urgent need for interventions and implementation strategies to optimize the use of CS while improving health outcomes and satisfaction in LMICs. This can only be achieved by engaging all stakeholders involved in the decision-making process surrounding birth and addressing their needs and concerns. The study will generate robust evidence about the effectiveness and the impact of this multifaceted intervention. It will also assess the acceptability and scalability of the intervention and the capacity for empowerment among women and providers alike.
Trial registration: ISRCTN67214403.
Keywords: Healthcare organization; Low- and middle-income countries; Nonclinical intervention; Quality of care; Shared decision-making; Unnecessary cesarean section.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Souza JP, Gulmezoglu A, Lumbiganon P, et al. Caesarean section without medical indications is associated with an increased risk of adverse short-term maternal outcomes: the 2004-2008 WHO Global Survey on Maternal and Perinatal Health. BMC Med. 2010;8:71. doi: 10.1186/1741-7015-8-71. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
