

PD1 Blockade Enhances ICAM1-Directed CAR T Therapeutic Efficacy in Advanced Thyroid Cancer
- PMID: 32887724
- PMCID: PMC7709864
- DOI: 10.1158/1078-0432.CCR-20-1523
PD1 Blockade Enhances ICAM1-Directed CAR T Therapeutic Efficacy in Advanced Thyroid Cancer
Abstract
Purpose: Advanced thyroid cancers, including poorly differentiated and anaplastic thyroid cancer (ATC), are lethal malignancies with limited treatment options. The majority of patients with ATC have responded poorly to programmed death 1 (PD1) blockade in early clinical trials. There is a need to explore new treatment options.
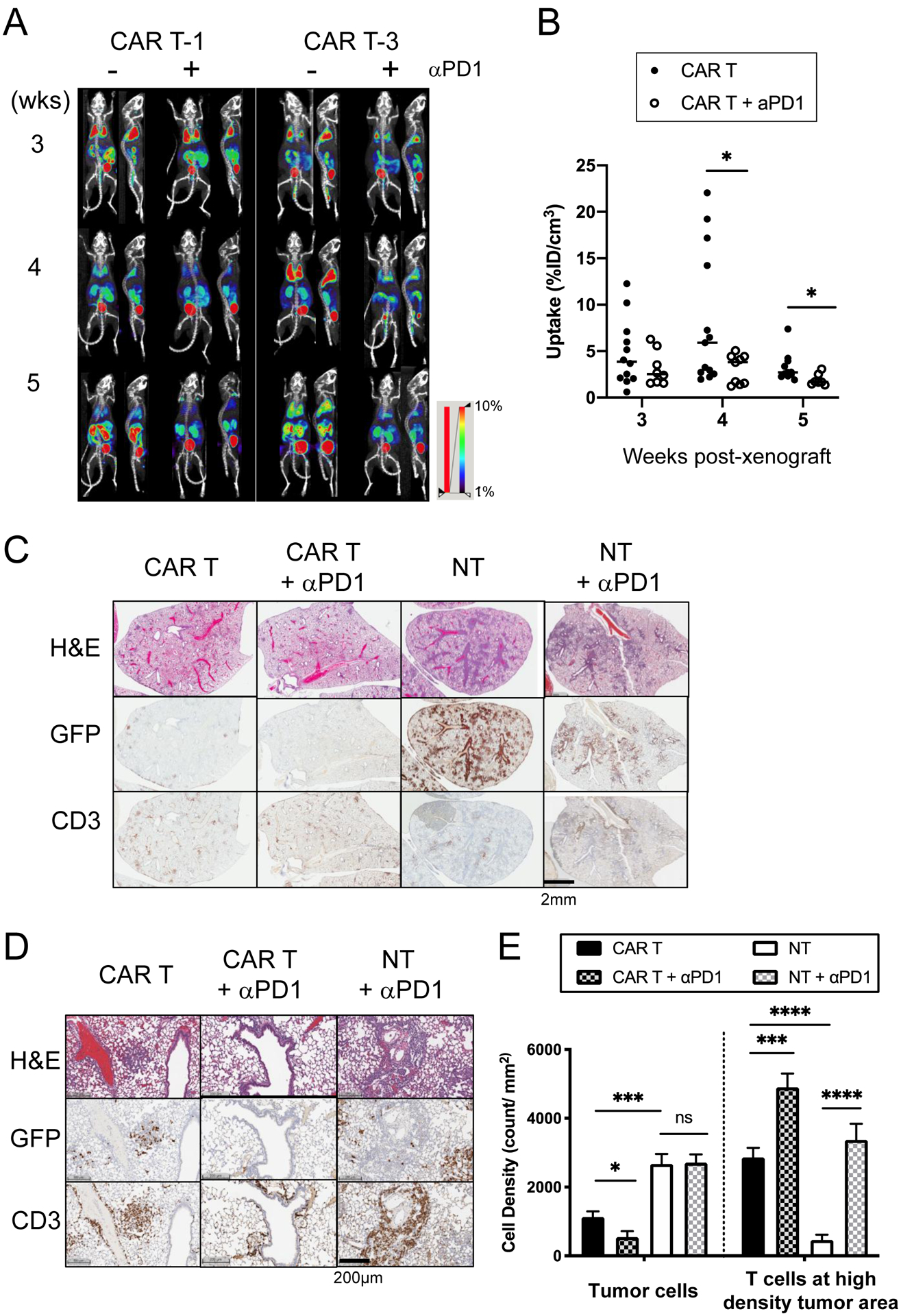
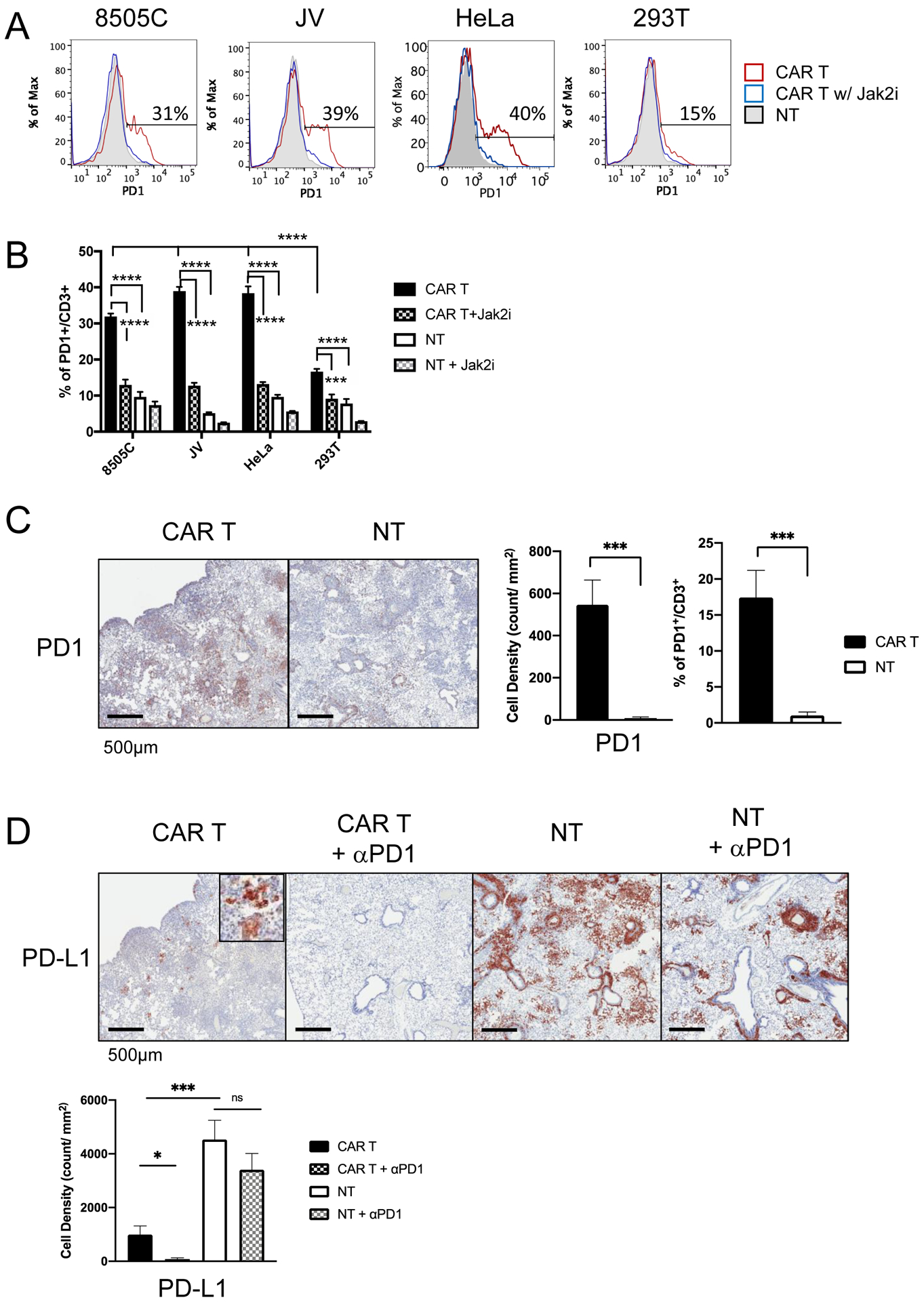
Experimental design: We examined the expression of PD-L1 (a ligand of PD1) and intercellular adhesion molecule 1 (ICAM1) in thyroid tumors and ATC cell lines, and investigated the PD1 expression level in peripheral T cells of patients with thyroid cancer. Next, we studied the tumor-targeting efficacy and T-cell dynamics of monotherapy and combination treatments of ICAM1-targeting chimeric antigen receptor (CAR) T cells and anti-PD1 antibody in a xenograft model of ATC.
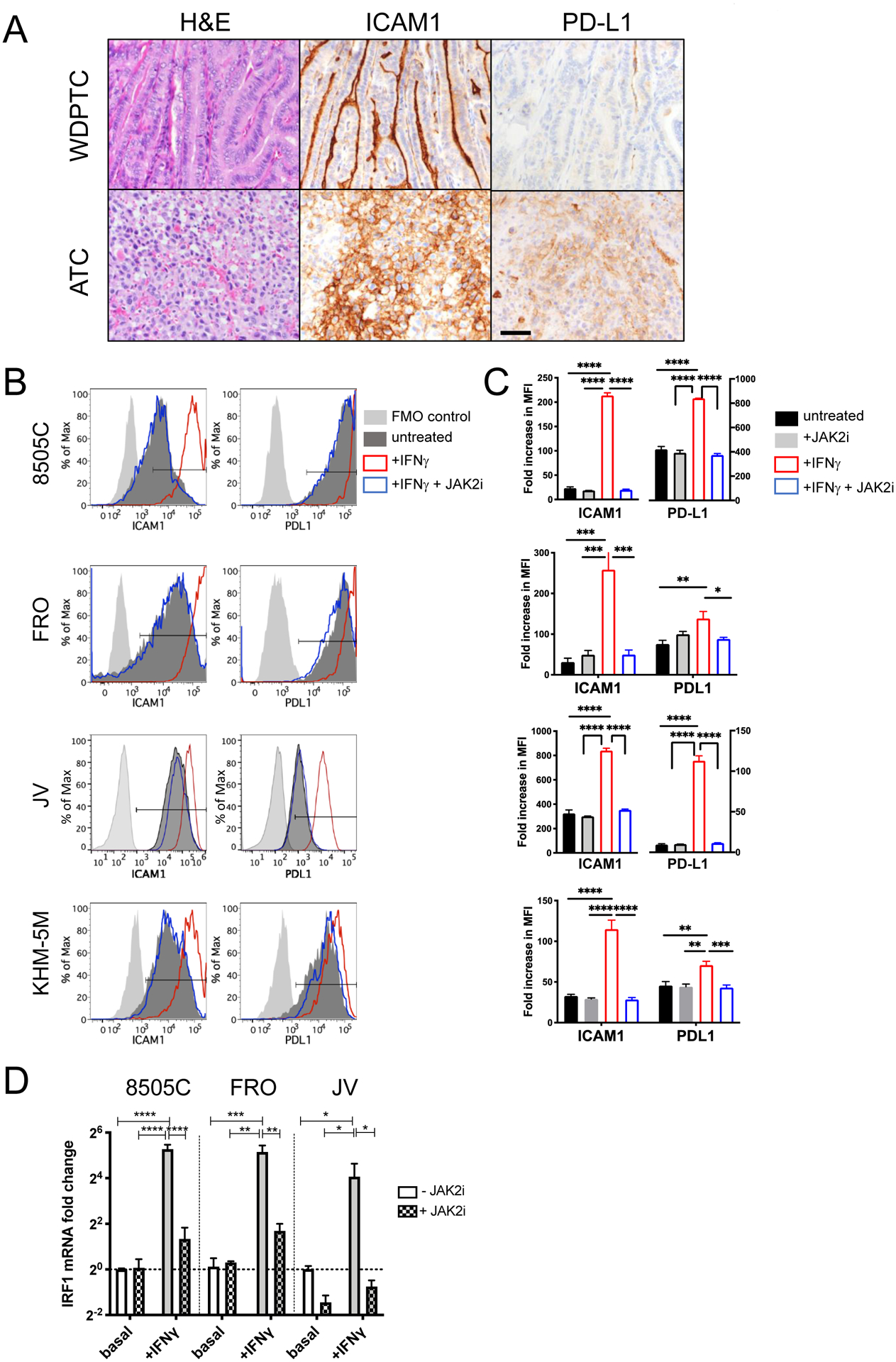
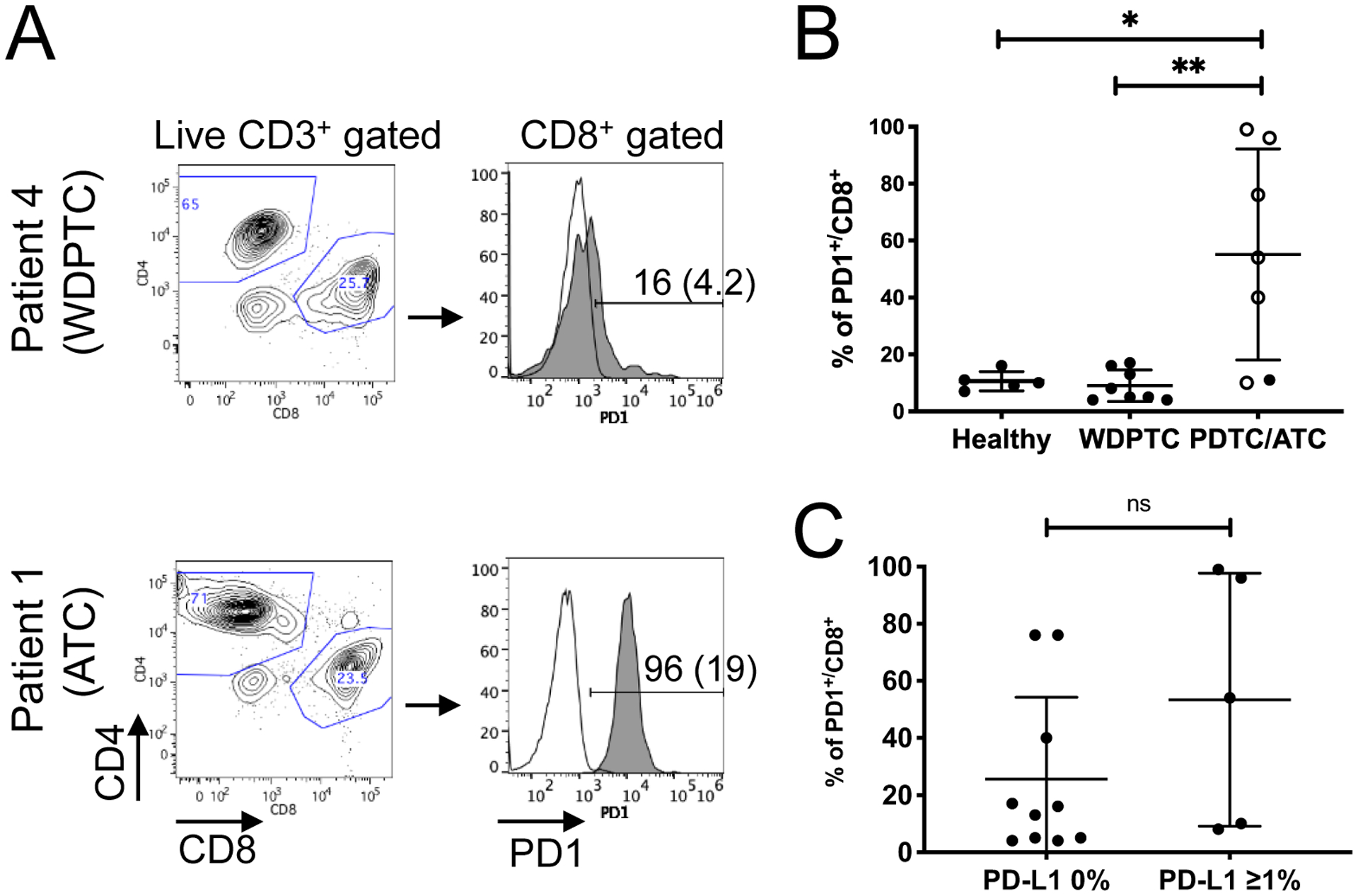
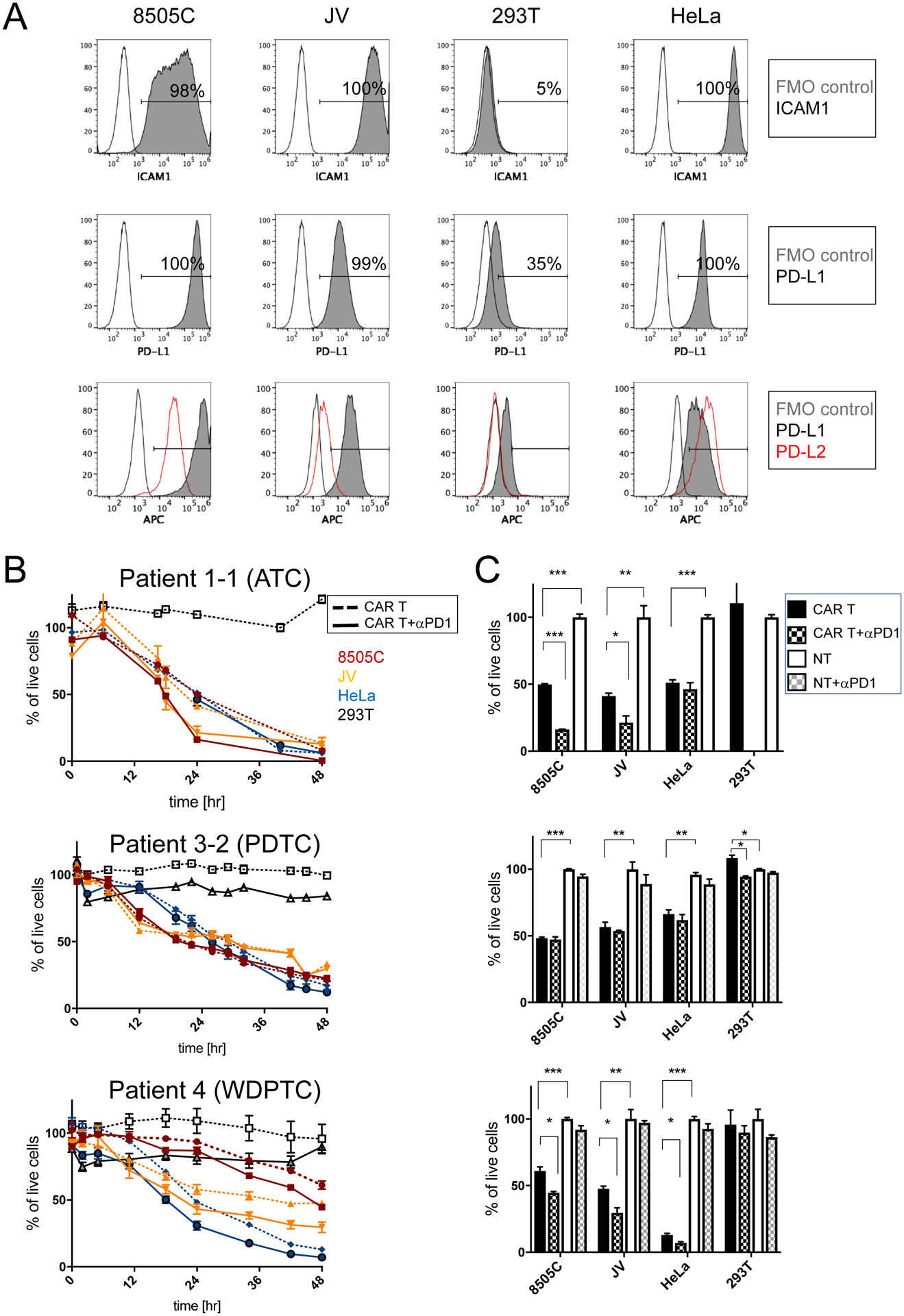
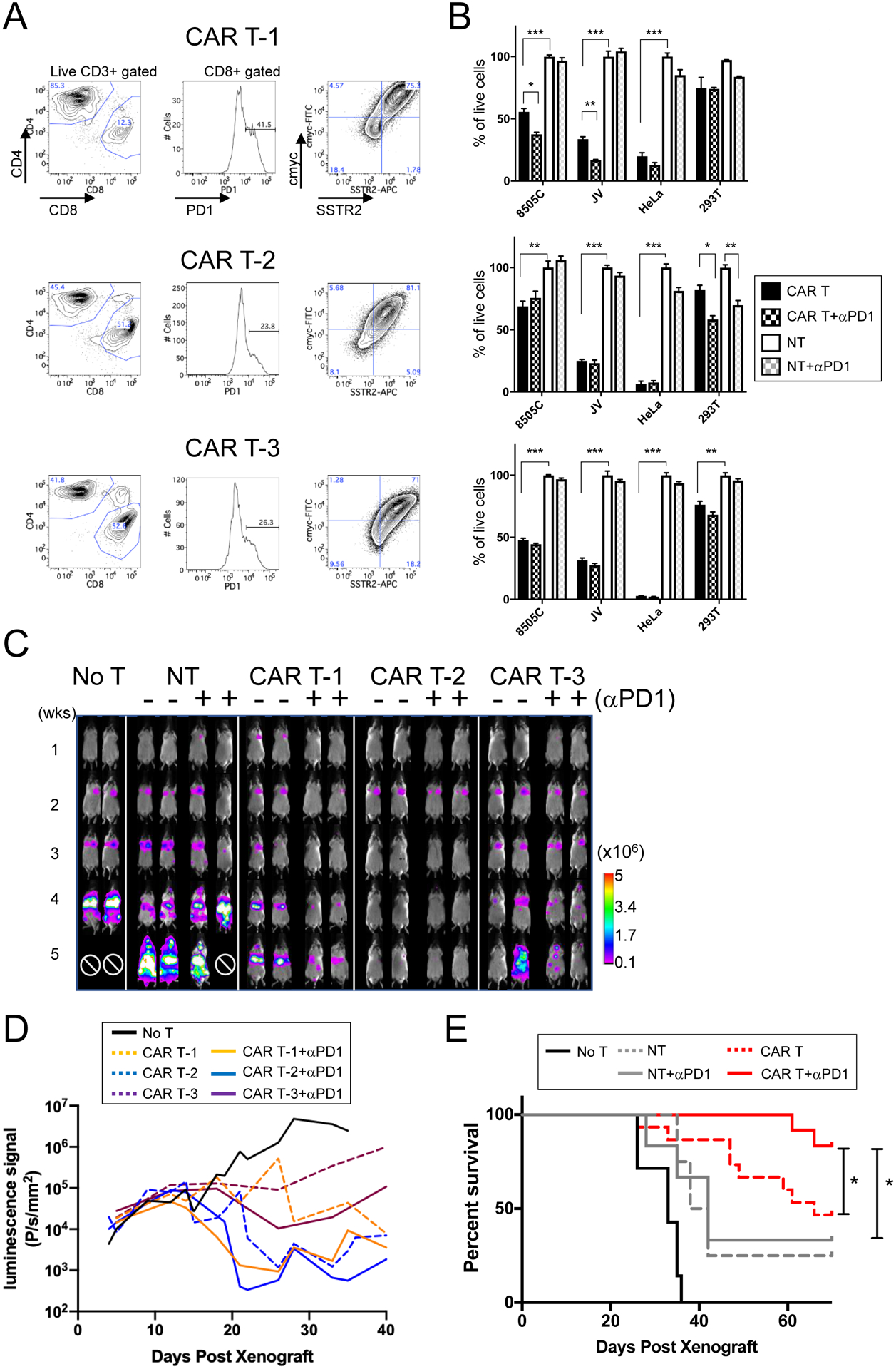
Results: Advanced thyroid cancers were associated with increased expression of both ICAM1 and PD-L1 in tumors, and elevated PD1 expression in CD8+ T cells of circulating blood. The expression of ICAM1 and PD-L1 in ATC lines was regulated by the IFNγ-JAK2 signaling pathway. ICAM1-targeted CAR T cells, produced from either healthy donor or patient T cells, in combination with PD1 blockade demonstrated an improved ability to eradicate ICAM1-expressing target tumor cells compared with CAR T treatment alone. PD1 blockade facilitated clearance of PD-L1 high tumor colonies and curtailed excessive CAR T expansion, resulting in rapid tumor clearance and prolonged survival in a mouse model.
Conclusions: Targeting two IFNγ-inducible, tumor-associated antigens-ICAM1 and PD-L1-in a complementary manner might be an effective treatment strategy to control advanced thyroid cancers in vivo.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
