

Elotuzumab, lenalidomide, and dexamethasone in RRMM: final overall survival results from the phase 3 randomized ELOQUENT-2 study
- PMID: 32887873
- PMCID: PMC7474076
- DOI: 10.1038/s41408-020-00357-4
Elotuzumab, lenalidomide, and dexamethasone in RRMM: final overall survival results from the phase 3 randomized ELOQUENT-2 study
Abstract
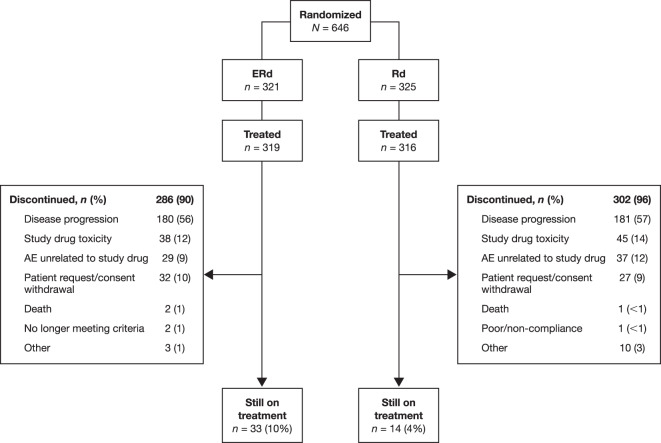
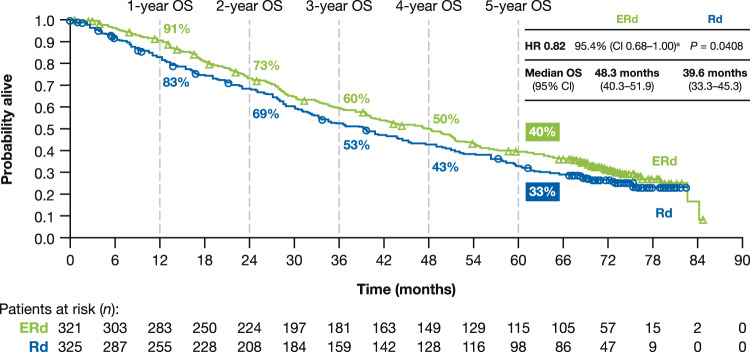
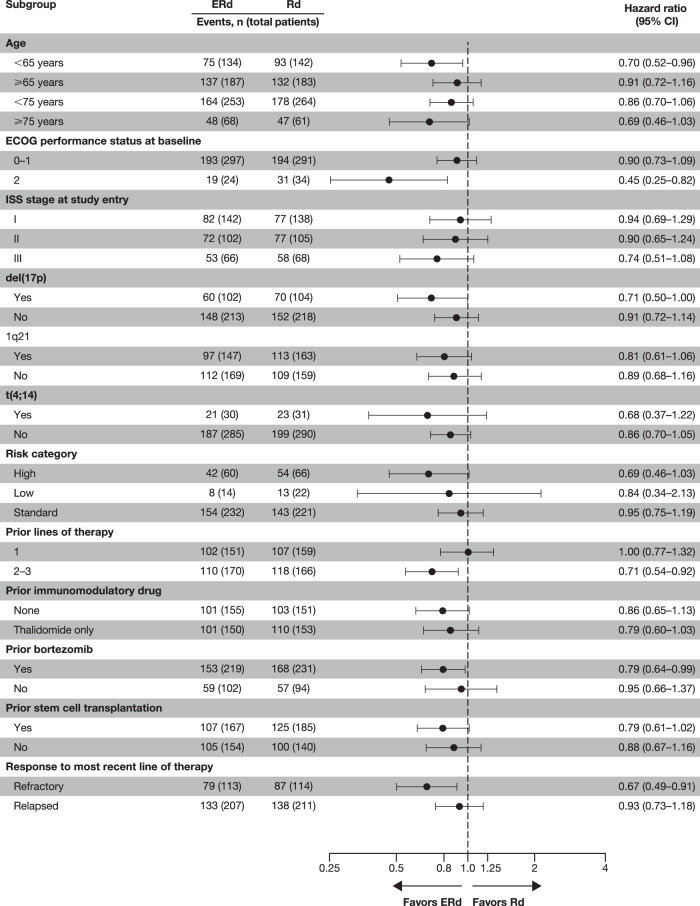
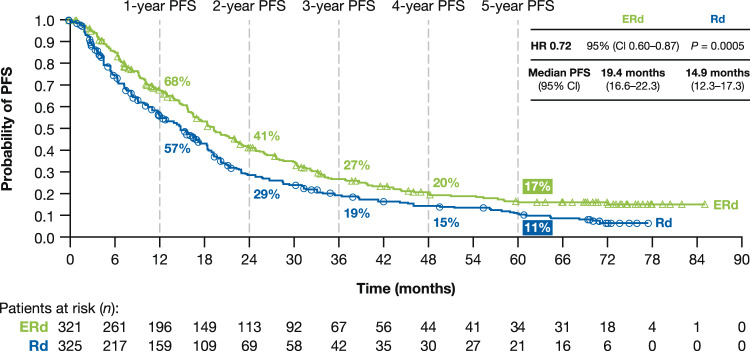
Prolonging overall survival (OS) remains an unmet need in relapsed or refractory multiple myeloma (RRMM). In ELOQUENT-2 (NCT01239797), elotuzumab plus lenalidomide/dexamethasone (ERd) significantly improved progression-free survival (PFS) versus lenalidomide/dexamethasone (Rd) in patients with RRMM and 1-3 prior lines of therapy (LoTs). We report results from the pre-planned final OS analysis after a minimum follow-up of 70.6 months, the longest reported for an antibody-based triplet in RRMM. Overall, 646 patients with RRMM and 1-3 prior LoTs were randomized 1:1 to ERd or Rd. PFS and overall response rate were co-primary endpoints. OS was a key secondary endpoint, with the final analysis planned after 427 deaths. ERd demonstrated a statistically significant 8.7-month improvement in OS versus Rd (median, 48.3 vs 39.6 months; hazard ratio, 0.82 [95.4% Cl, 0.68-1.00]; P = 0.0408 [less than allotted α of 0.046]), which was consistently observed across key predefined subgroups. No additional safety signals with ERd at extended follow-up were reported. ERd is the first antibody-based triplet regimen shown to significantly prolong OS in patients with RRMM and 1-3 prior LoTs. The magnitude of OS benefit was greatest among patients with adverse prognostic factors, including older age, ISS stage III, IMWG high-risk disease, and 2-3 prior LoTs.
Conflict of interest statement
M.A.D.: Honoraria and consultancy: Amgen, Bristol-Myers Squibb Company, Celgene, Janssen, Takeda. S.L.: Consultancy: AbbVie, Amgen, Bristol-Myers Squibb Company, Celgene, GlaxoSmithKline, Janssen, Merck, Takeda. Research support: Celgene, Janssen, Takeda. D.W.: Honoraria, consultancy/advisory role: Amgen, Antengene, Celgene, Janssen, Sanofi, Takeda. P.M.: Advisory boards and honoraria: AbbVie, Amgen, Celgene, Janssen, Takeda. K.W.: Honoraria: Amgen, Adaptive Biotech, Bristol-Myers Squibb Company, Celgene, GlaxoSmithKline, Janssen, Karyopharm, Novartis, Sanofi, Takeda. Research funding (institution): Amgen, Celgene, Janssen, Sanofi. Advisory board fees: Amgen, Adaptive Biotech, Bristol-Myers Squibb Company, Celgene, Janssen, Juno, Sanofi, Takeda during the conduct of the study. J.S-M.: Advisory board: AbbVie, Amgen, Bristol-Myers Squibb Company, Celgene, MSD, Novartis, Roche, Sanofi, Takeda. O.S.: Consultancy/advisory role: Gilead, Millennium/Takeda. S.G.: Nothing to disclose. I.Š.: Honoraria: Amgen, Celgene, Janssen-Cilag, Novartis, Takeda. Consulting fees: Amgen, Celgene, Janssen-Cilag, Novartis, Sanofi, Takeda. Lecture fees: Amgen, Bristol-Myers Squibb Company, Celgene, Janssen-Cilag, Novartis, Sanofi, Takeda. A.W-C.: Consultancy/advisory role: Janssen. H.M.: Nothing to disclose. M-V.M.: Honoraria/advisory boards: AbbVie, Adaptive Biotech, Amgen, Celgene, GlaxoSmithKline, Janssen, Mundipharma EDO, Pharmamar, Takeda. A.B.: Nothing to disclose. D.R.: Research funding: Amgen, Bristol-Myers Squibb Company, Celgene, Janssen, Takeda. Consultancy: Amgen, Celgene, Janssen, Karyopharm, Takeda. Honoraria: Amgen, Celgene, Janssen, Takeda. Expert testimony at Health Canada: Amgen, Celgene, Janssen. Advisory board: Celgene, Janssen, Karyopharm. M.B.: Speakers bureau: Celgene, Janssen. Advisory board: Celgene, Janssen, Sanofi, Takeda. A.S.: Consultancy: AbbVie, Celgene, Haemalogix, Janssen, Sanofi, Secura Bio, Servier, Specialized Therapeutics Australia. Speakers bureau: Celgene, Janssen, Takeda. Grant/research support: Amgen, Celgene, Haemalogix, Janssen, Servier, Takeda. Honoraria: AbbVie, Amgen, Celgene, Haemalogix, Janssen, Sanofi, Secura Bio, Servier, Specialized Therapeutics Australia, Takeda. H.O.: Conference sponsorship: Takeda. Advisory board/sponsorship: Bristol-Myers Squibb Company, Janssen, Novartis. M.T.: Honoraria: Bristol-Myers Squibb K.K., Celgene. Research funding: Astellas, Chugai, Daiichi Sankyo, MSD. R.Z.O.: Advisory boards with honoraria: Bristol-Myers Squibb Company, Celgene, FORMA Therapeutics, Ioni Pharmaceuticals, Legend Biotech, Millennium/Takeda, Molecular Partners, Onyx Pharmaceuticals/Amgen, Sanofi-Aventis, Servier, Takeda. Advisory boards without honoraria: Acetylon Pharmaceuticals. Grant/research funding: BioTheryX, Bristol-Myers Squibb Company, Celgene, Karus Pharmaceuticals, Millennium/Takeda, Onyx Pharmaceuticals/Amgen, Spectrum Pharmaceuticals C.R.: Honoraria, consultancy/advisory role: AbbVie, Amgen, Astellas, Bristol-Myers Squibb Company, Celgene, Daiichy Sankyo, Janssen, Jazz, Novartis, Pfizer, Roche. Research funding: AbbVie, Amgen, Bayer, Celgene, Janssen, Jazz, Novartis, Pfizer, Roche. H.E.: Grants: Amgen, Bristol-Myers Squibb Company, Celgene, Janssen. Honoraria: Amgen, Bristol-Myers Squibb Company, Celgene, Janssen, Novartis, Takeda. Advisory boards: Amgen, Bristol-Myers Squibb Company, Celgene, Janssen, Novartis, Takeda. M.M.: Honoraria: Bristol-Myers Squibb K.K. K.L.W.: Consultancy/advisory role: Amgen, Celgene, Janssen-Cilag, Takeda. K.C.A.: Advisory boards: Bristol-Myers Squibb Company, Celgene, Gilead, Janssen, Millennium, Sanofi-Aventis. A.G.: Employment: Bristol-Myers Squibb Company. Y-M.J.: Employment and stock: Bristol-Myers Squibb Company. A.K.S.: Employee at time of study: AbbVie. P.G.R.: Research support: Bristol-Myers Squibb Company, Celgene, Oncopeptides, Takeda. Advisory boards: Amgen, Celgene, Janssen, Karyopharm, Oncopeptides, Sanofi, Takeda.
Figures
References
-
- Howlader, N. et al. SEER Cancer Statistics Review, 1975–2016. Bethesda, MD; 2019.
-
- Usmani S, et al. Analysis of real-world data on overall survival in multiple myeloma patients with ≥3 prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory drug (IMiD), or double refractory to a PI and an IMiD. Oncologist. 2016;21:1355–1361. doi: 10.1634/theoncologist.2016-0104. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
