

Characteristics and predictors of hospitalization and death in the first 11 122 cases with a positive RT-PCR test for SARS-CoV-2 in Denmark: a nationwide cohort
- PMID: 32887982
- PMCID: PMC7499657
- DOI: 10.1093/ije/dyaa140
Characteristics and predictors of hospitalization and death in the first 11 122 cases with a positive RT-PCR test for SARS-CoV-2 in Denmark: a nationwide cohort
Abstract
Background: Population-level knowledge on individuals at high risk of severe and fatal coronavirus disease 2019 (COVID-19) is urgently needed to inform targeted protection strategies in the general population.
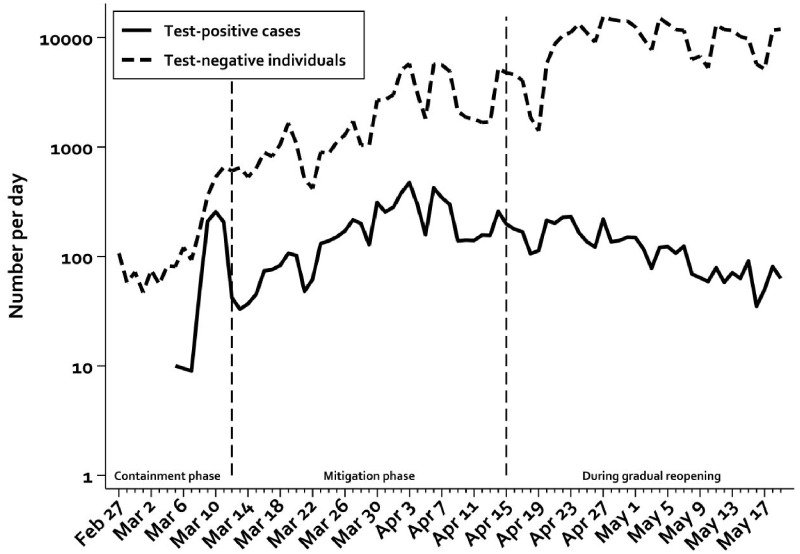
Methods: We examined characteristics and predictors of hospitalization and death in a nationwide cohort of all Danish individuals tested for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from 27 February 2020 until 19 May 2020.
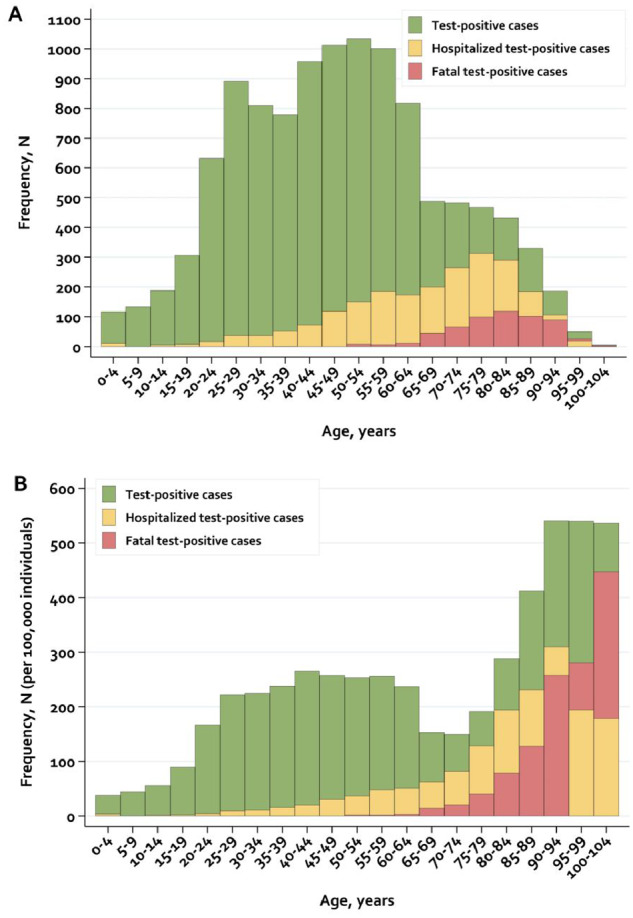
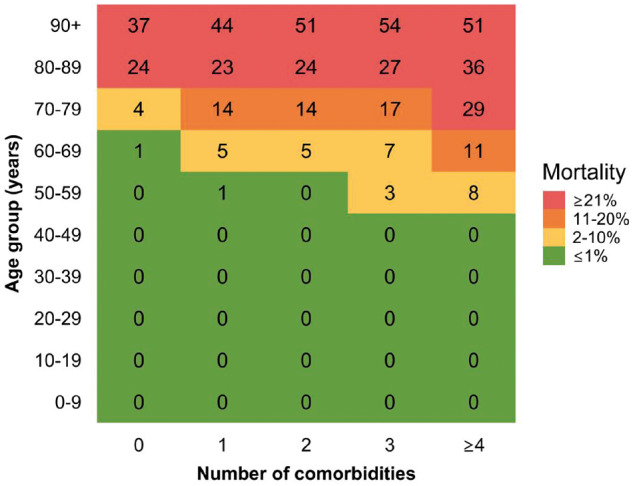
Results: We identified 11 122 SARS-CoV-2 polymerase chain reaction-positive cases of whom 80% were community-managed and 20% were hospitalized. Thirty-day all-cause mortality was 5.2%. Age was strongly associated with fatal disease {odds ratio [OR] 15 [95% confidence interval (CI): 9-26] for 70-79 years, increasing to OR 90 (95% CI: 50-162) for ≥90 years, when compared with cases aged 50-59 years and adjusted for sex and number of co-morbidities}. Similarly, the number of co-morbidities was associated with fatal disease [OR 5.2 (95% CI: 3.4-8.0), for cases with at least four co-morbidities vs no co-morbidities] and 79% of fatal cases had at least two co-morbidities. Most major chronic diseases were associated with hospitalization, with ORs ranging from 1.3-1.4 (e.g. stroke, ischaemic heart disease) to 2.6-3.4 (e.g. heart failure, hospital-diagnosed kidney disease, organ transplantation) and with mortality with ORs ranging from 1.1-1.3 (e.g. ischaemic heart disease, hypertension) to 2.5-3.2 (e.g. major psychiatric disorder, organ transplantation). In the absence of co-morbidities, mortality was <5% in persons aged ≤80 years.
Conclusions: In this nationwide population-based COVID-19 study, increasing age and multimorbidity were strongly associated with hospitalization and death. In the absence of co-morbidities, the mortality was, however, <5% until the age of 80 years.
Keywords: COVID-19; SARS-CoV-2; death; epidemiology; hospitalization; infectious disease; population-based; predictors.
© The Author(s) 2020. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- Johns Hopkins Coronavirus Resource Center. Johns Hopkins Coronavirus Resource Center. https://coronavirus.jhu.edu/ (16 April 2020, date last accessed).
-
- COVID-19 i Danmark. Epidemiologisk overvågningsrapport. https://www.ssi.dk/aktuelt/sygdomsudbrud/coronavirus/covid-19-i-danmark-... (28 July 2020, date last accessed).
-
- Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA 2020;doi:10.1001/jama.2020.4683. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
