

Molecular profiling of neuroendocrine tumours to predict response and toxicity to peptide receptor radionuclide therapy
- PMID: 32888472
- PMCID: PMC8385643
- DOI: 10.1016/S1470-2045(20)30323-5
Molecular profiling of neuroendocrine tumours to predict response and toxicity to peptide receptor radionuclide therapy
Abstract
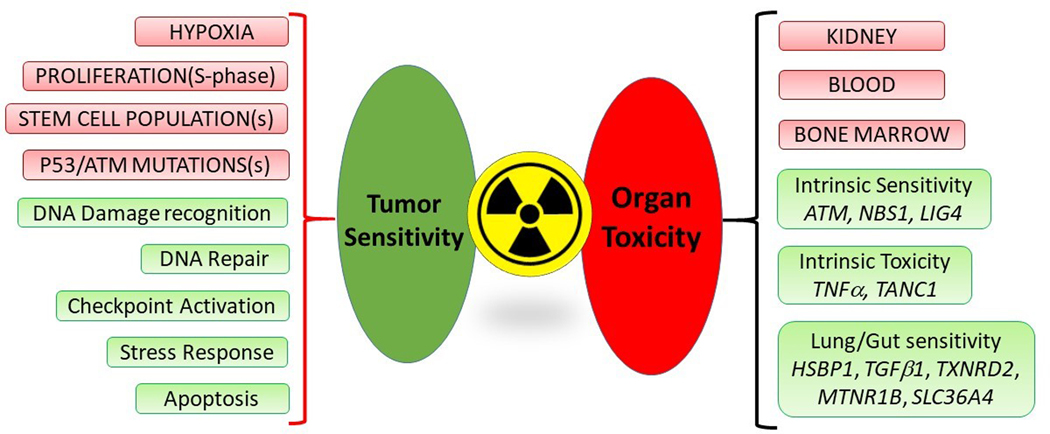
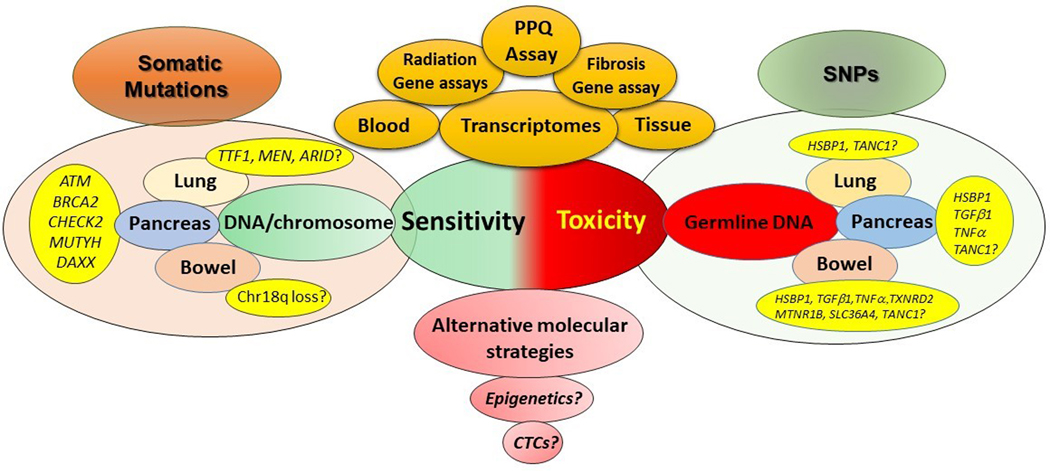
Peptide receptor radionuclide therapy (PRRT) is a type of radiotherapy that targets peptide receptors and is typically used for neuroendocrine tumours (NETs). Some of the key challenges in its use are the prediction of efficacy and toxicity, patient selection, and response optimisation. In this Review, we assess current knowledge on the molecular profile of NETs and the strategies and tools used to predict, monitor, and assess the toxicity of PRRT. The few mutations in tumour genes that can be evaluated (eg, ATM and DAXX) are limited to pancreatic NETs and are most likely not informative. Assays that are transcriptomic or based on genes are effective in the prediction of radiotherapy response in other cancers. A blood-based assay for eight genes (the PRRT prediction quotient [PPQ]) has an overall accuracy of 95% for predicting responses to PRRT in NETs. No molecular markers exist that can predict the toxicity of PRRT. Candidate molecular targets include seven single nucleotide polymorphisms (SNPs) that are susceptible to radiation. Transcriptomic evaluations of blood and a combination of gene expression and specific SNPs, assessed by machine learning with algorithms that are tumour-specific, might yield molecular tools to enhance the efficacy and safety of PRRT.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflicts of interest
LB – grants and non-financial support from AAA-Novartis, non-financial support from Ipsen, non-financial support from Clovis Oncology, non-financial support from Curium.
RPB – Consultancy fees from ITG Isotope Technologies Garching, Ipsen Pharma, Novartis. He is shareholder of Telix Pharma, Clovis Oncology, BAMF Health and consultant/advisor of OctreoPharm Sciences GmbH, Advanced Accelerator Applications, and 1717 LSV.
KH – Consultancy fees from Endocyte, Bayer, Ipsen, AAA, Novartis, BTG, Sirtex, Curium, Amgen, Siemens Healthineers, GE Healthcare, Ymabs. Shareholder of Sofie Biosciences. Non-financial support from ABX. Grant support from BTG.
JS – Consultancy and speaker bureau from Lexicon, Ipsen, and Novartis, outside the submitted work
MC – Consultancy fees and Speaker honoraria from AAA, Ipsen, Novartis, Pfizer (all outside the submitted work).
IMM – Medical and scientific consultant for Wren Laboratories.
The other authors declared no conflicts of interest.
Figures

References
-
- Kwekkeboom DJ, de Herder WW, Kam BL, et al.Treatment with the radiolabeled somatostatin analog [177 Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol 2008; 26(13): 2124–30. - PubMed
-
- Kwekkeboom DJ, Kam BL, van Essen M, et al.Somatostatin-receptor-based imaging and therapy of gastroenteropancreatic neuroendocrine tumors. Endocr Relat Cancer 2010; 17(1): R53–73. Print 2010 Mar. - PubMed
-
- Baum RP, Kulkarni HR, Singh A, et al.Results and adverse events of personalized peptide receptor radionuclide therapy with (90)Yttrium and (177)Lutetium in 1048 patients with neuroendocrine neoplasms. Oncotarget 2018; 9(24): 16932–50. doi: 10.8632/oncotarget.24524. eCollection 2018 Mar 30. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
