

Histopathology-validated recommendations for cortical lesion imaging in multiple sclerosis
- PMID: 32889535
- PMCID: PMC7586087
- DOI: 10.1093/brain/awaa233
Histopathology-validated recommendations for cortical lesion imaging in multiple sclerosis
Abstract
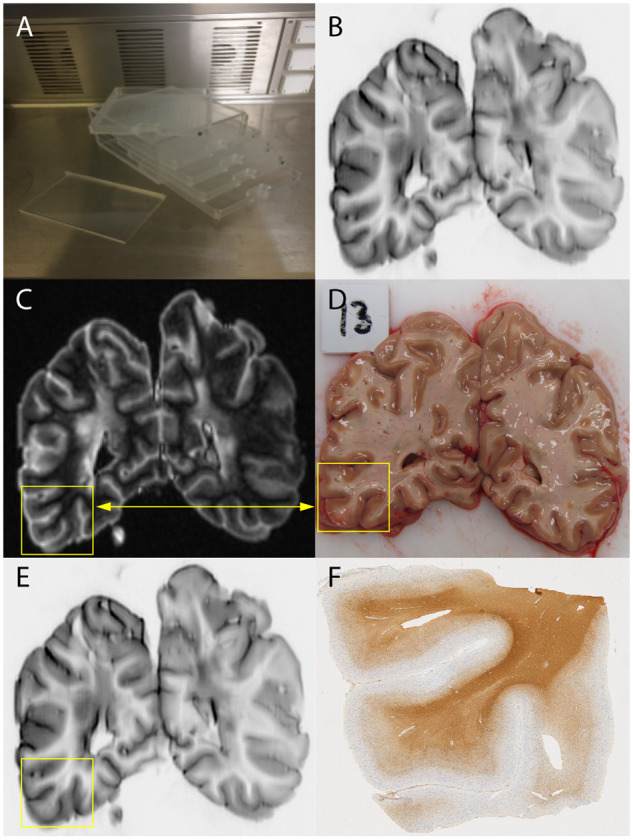
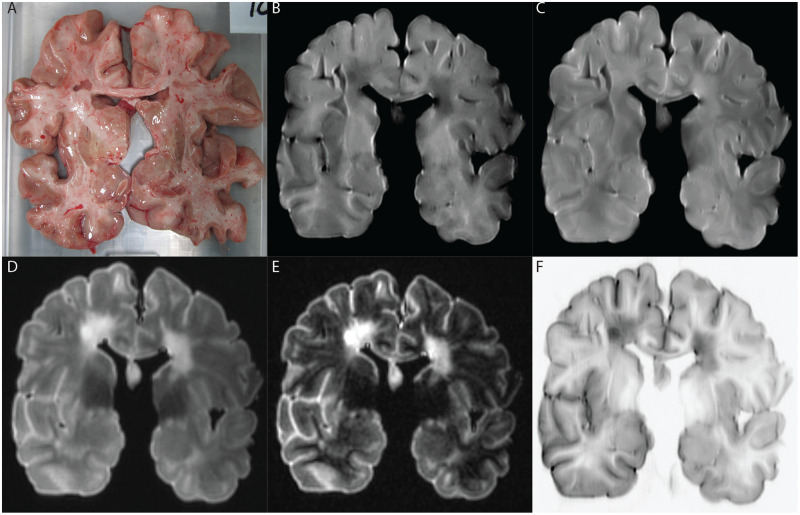
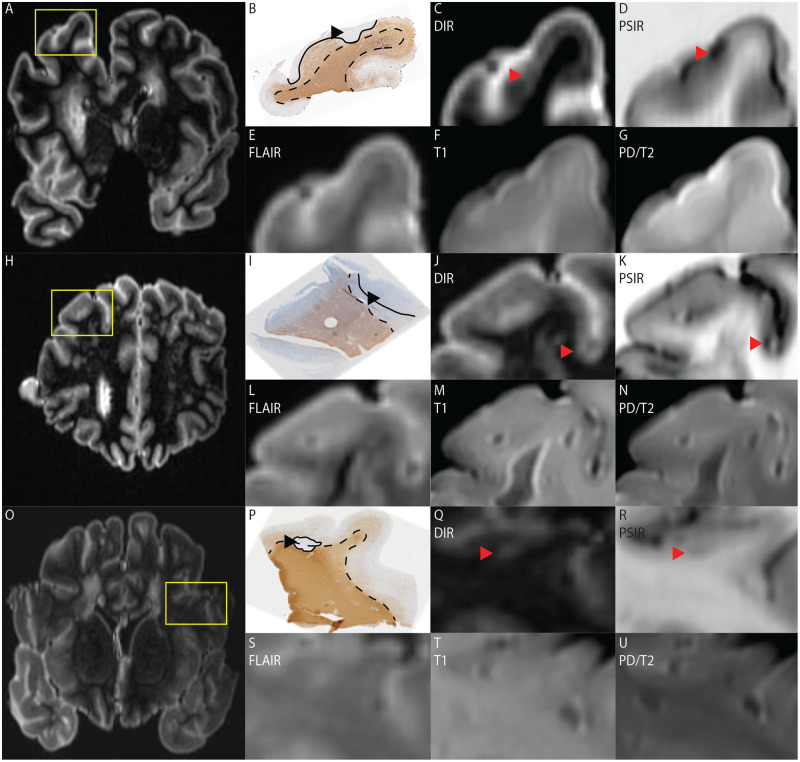
Cortical demyelinating lesions are clinically important in multiple sclerosis, but notoriously difficult to visualize with MRI. At clinical field strengths, double inversion recovery MRI is most sensitive, but still only detects 18% of all histopathologically validated cortical lesions. More recently, phase-sensitive inversion recovery was suggested to have a higher sensitivity than double inversion recovery, although this claim was not histopathologically validated. Therefore, this retrospective study aimed to provide clarity on this matter by identifying which MRI sequence best detects histopathologically-validated cortical lesions at clinical field strength, by comparing sensitivity and specificity of the thus far most commonly used MRI sequences, which are T2, fluid-attenuated inversion recovery (FLAIR), double inversion recovery and phase-sensitive inversion recovery. Post-mortem MRI was performed on non-fixed coronal hemispheric brain slices of 23 patients with progressive multiple sclerosis directly after autopsy, at 3 T, using T1 and proton-density/T2-weighted, as well as FLAIR, double inversion recovery and phase-sensitive inversion recovery sequences. A total of 93 cortical tissue blocks were sampled from these slices. Blinded to histopathology, all MRI sequences were consensus scored for cortical lesions. Subsequently, tissue samples were stained for proteolipid protein (myelin) and scored for cortical lesion types I-IV (mixed grey matter/white matter, intracortical, subpial and cortex-spanning lesions, respectively). MRI scores were compared to histopathological scores to calculate sensitivity and specificity per sequence. Next, a retrospective (unblinded) scoring was performed to explore maximum scoring potential per sequence. Histopathologically, 224 cortical lesions were detected, of which the majority were subpial. In a mixed model, sensitivity of T1, proton-density/T2, FLAIR, double inversion recovery and phase-sensitive inversion recovery was 8.9%, 5.4%, 5.4%, 22.8% and 23.7%, respectively (20, 12, 12, 51 and 53 cortical lesions). Specificity of the prospective scoring was 80.0%, 75.0%, 80.0%, 91.1% and 88.3%. Sensitivity and specificity did not significantly differ between double inversion recovery and phase-sensitive inversion recovery, while phase-sensitive inversion recovery identified more lesions than double inversion recovery upon retrospective analysis (126 versus 95; P < 0.001). We conclude that, at 3 T, double inversion recovery and phase-sensitive inversion recovery sequences outperform conventional sequences T1, proton-density/T2 and FLAIR. While their overall sensitivity does not exceed 25%, double inversion recovery and phase-sensitive inversion recovery are highly pathologically specific when using existing scoring criteria and their use is recommended for optimal cortical lesion assessment in multiple sclerosis.
Keywords: cortical lesions; double inversion recovery; multiple sclerosis; phase-sensitive inversion recovery; post-mortem imaging.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Barkhof F. The clinico-radiological paradox in multiple sclerosis revisited. Curr Opin Neurol 2002; 15: 239–45. - PubMed
-
- Barkhof F, Geurts JJ.. Laminar cortical damage in multiple sclerosis. Brain 2015; 138: 828–9. - PubMed
-
- Bö L, Geurts JJG, Ravid R, Barkhof F.. Magnetic resonance imaging as a tool to examine the neuropathology of multiple sclerosis. Neuropathol Appl Neurobiol 2004; 30: 106–17. - PubMed
-
- Bø L, Vedeler CA, Nyland HI, Trapp BD, Mørk SJ.. Subpial demyelination in the cerebral cortex of multiple sclerosis patients. J Neuropathol Exp Neurol 2003; 62: 723–32. - PubMed
-
- Calabrese M, Agosta F, Rinaldi F, Mattisi I, Grossi P, Favaretto A, et al. Cortical lesions and atrophy associated with cognitive impairment in relapsing-remitting multiple sclerosis. Arch Neurol 2009; 66: 1144–50. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
