

Lymph node response to chemoradiotherapy in oesophageal cancer patients: relationship with radiotherapy fields
- PMID: 32889674
- PMCID: PMC7794105
- DOI: 10.1007/s10388-020-00777-y
Lymph node response to chemoradiotherapy in oesophageal cancer patients: relationship with radiotherapy fields
Abstract
Background: The presence of lymph node metastasis (LNmets) is a poor prognostic factor in oesophageal cancer (OeC) patients treated with neoadjuvant chemoradiotherapy (nCRT) followed by surgery. Tumour regression grade (TRG) in LNmets has been suggested as a predictor for survival. The aim of this study was to investigate whether TRG in LNmets is related to their location within the radiotherapy (RT) field.
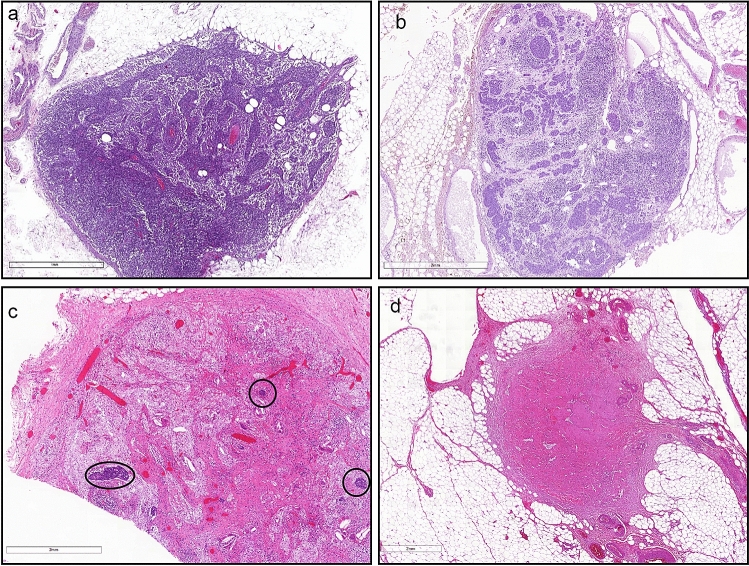
Methods: Histopathological TRG was retrospectively classified in 2565 lymph nodes (LNs) from 117 OeC patients treated with nCRT and surgery as: (A) no tumour, no signs of regression; (B) tumour without regression; (C) viable tumour and regression; and (D) complete response. Multivariate survival analysis was used to investigate the relationship between LN location within the RT field, pathological TRG of the LN and TRG of the primary tumour.
Results: In 63 (54%) patients, viable tumour cells or signs of regression were seen in 264 (10.2%) LNs which were classified as TRG-B (n = 56), C (n = 104) or D (n = 104) LNs. 73% of B, C and D LNs were located within the RT field. There was a trend towards a relationship between LN response and anatomical LN location with respect to the RT field (p = 0.052). Multivariate analysis showed that only the presence of LNmets within the RT field with TRG-B is related to poor overall survival.
Conclusion: Patients have the best survival if all LNmets show tumour regression, even if LNmets are located outside the RT field. Response in LNmets to nCRT is heterogeneous which warrants further studies to better understand underlying mechanisms.
Keywords: Lymph node regression; Neoadjuvant chemoradiotherapy; Oesophageal cancer; Radiation field.
Conflict of interest statement
All authors declare to have no conflict of interest.
Figures




References
-
- Lordick F, Mariette C, Haustermans K, Obermannova R, Arnold D. Oesophageal cancer: eSMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2016;27(suppl 5):v50–v57. - PubMed
-
- van Hagen P, Hulshof MC, van Lanschot JJ, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074–2084. - PubMed
-
- Allum WH, Stenning SP, Bancewicz J, Clark PI, Langley RE. Long-term results of a randomized trial of surgery with or without preoperative chemotherapy in esophageal cancer. J Clin Oncol. 2009;27(30):5062–5067. - PubMed
-
- Shapiro J, van Lanschot JJB, Hulshof M, et al. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16(9):1090–1098. - PubMed
-
- Mandard AM, Dalibard F, Mandard JC, et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer. 1994;73(11):2680–2686. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical