

Intensive statin versus low-dose statin + ezetimibe treatment for fibrous cap thickness of coronary vulnerable plaques
- PMID: 32889912
- PMCID: PMC7575174
- DOI: 10.1097/CM9.0000000000001067
Intensive statin versus low-dose statin + ezetimibe treatment for fibrous cap thickness of coronary vulnerable plaques
Abstract
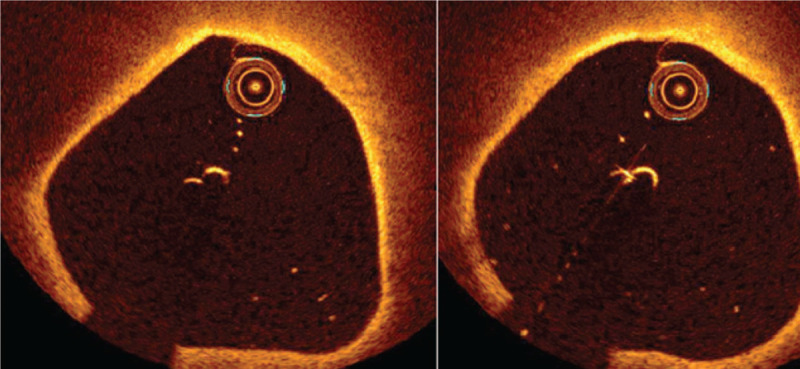
Background: Acute coronary syndromes mainly result from abrupt thrombotic occlusion caused by atherosclerotic vulnerable plaques (VPs) that suddenly rupture or erosion. Fibrous cap thickness (FCT) is a major determinant of the propensity of a VP to rupture and is recognized as a key factor. The intensive use of statins is known to have the ability to increase FCT; however, there is a risk of additional adverse effects. However, lower dose statin with ezetimibe is known to be tolerable by patients. The present study aimed to investigate the effect of intensive statin vs. low-dose stain + ezetimibe therapy on FCT, as evaluated using optical coherence tomography.
Method: Patients who had VPs (minimum FCT <65 μm and lipid core >90°) and deferred from intervention in our single center from January 2014 to December 2018 were included in the trial. They were divided into the following two groups: intensive statin group (rosuvastatin 15-20 mg or atorvastatin 30-40 mg) and combination therapy group (rosuvastatin 5-10 mg or atorvastatin 10-20 mg + ezetimibe 10 mg). At the 12-month follow-up, we compared the change in the FCT (ΔFCT%) between the two groups and analyzed the association of ΔFCT% with risk factors. Fisher exact test was used for all categorical variables. Student's t test or Mann-Whitney U-test was used for analyzing the continuous data. The relationship between ΔFCT% and risk factors was analyzed using linear regression analysis.
Result: Total 53 patients were finally enrolled, including 26 patients who were in the intensive statin group and 27 who were in the combination therapy group. At the 12-month follow-up, the serum levels of total cholesterol (TC), total triglyceride, low-density lipoprotein (LDL-C), hypersensitive C-reactive protein (hs-CRP), and lipoprotein-associated phospholipase A2 (Lp-PLA2) levels were reduced in both the groups. The ΔTC%, ΔLDL-C%, and ΔLp-PLA2% were decreased further in the combination therapy group. FCT was increased in both the groups (combination treatment group vs. intensive statin group: 128.89 ± 7.64 vs. 110.19 ± 7.00 μm, t = -9.282, P < 0.001) at the 12-month follow-up. The increase in ΔFCT% was more in the combination therapy group (123.46% ± 14.05% vs. 91.14% ± 11.68%, t = -9.085, P < 0.001). Based on the multivariate linear regression analysis, only the serum Lp-PLA2 at the 12-month follow-up (B = -0.203, t = -2.701, P = 0.010), ΔTC% (B = -0.573, t = -2.048, P = 0.046), and Δhs-CRP% (B = -0.302, t = -2.963, P = 0.005) showed an independent association with ΔFCT%.
Conclusions: Low-dose statin combined with ezetimibe therapy maybe provide a profound and significant increase in FCT as compared to intensive statin monotherapy. The reductions in Lp-PLA2, ΔTC%, and Δhs-CRP% are independently associated with an increase in FCT.
Conflict of interest statement
None.
Figures

References
-
- Johnson TW, Räber L, di Mario C, Bourantas C, Jia H, Mattesini A, et al. Clinical use of intracoronary imaging. Part 2: acute coronary syndromes, ambiguous coronary angiography findings, and guiding interventional decision-making: an expert consensus document of the European Association of Percutaneous Cardiovascular Interventions. Eur Heart J 2019; 40:2566–2584. doi: 10.1093/eurheartj/ehz332. - PubMed
-
- Sugiyama T, Yamamoto E, Bryniarski K, Xing L, Lee H, Isobe M, et al. Nonculprit plaque characteristics in patients with acute coronary syndrome caused by plaque erosion vs plaque rupture: a 3-vessel optical coherence tomography study. JAMA Cardiol 2018; 3:207–214. doi: 10.1001/jamacardio.2017.5234. - PMC - PubMed
-
- Stone GW, Maehara A, Lansky AJ, de Bruyne B, Cristea E, Mintz GS, et al. A prospective natural history study of coronary atherosclerosis. N Engl J Med 2011; 364:226–235. doi: 10.1056/NEJMoa1002358. - PubMed
-
- Arbab-Zadeh A, Fuster V. From detecting the vulnerable plaque to managing the vulnerable patient: JACC state-of-the-art review. J Am Coll Cardiol 2019; 74:1582–1593. doi: 10.1016/j.jacc.2019.07.062. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
