

Resistance Exercise Dosage in Men with Prostate Cancer: Systematic Review, Meta-analysis, and Meta-regression
- PMID: 32890199
- PMCID: PMC7886340
- DOI: 10.1249/MSS.0000000000002503
Resistance Exercise Dosage in Men with Prostate Cancer: Systematic Review, Meta-analysis, and Meta-regression
Abstract
Purpose: Resistance exercise improves an array of treatment-related adverse effects in men with prostate cancer; however, the minimal dosage required is unknown. We systematically reviewed the resistance training effects in prostate cancer patients to determine the minimal dosage regarding the exercise components (type, duration, volume, and intensity) on body composition, physical function, muscle strength, cardiorespiratory fitness, body mass index, and prostate-specific antigen.
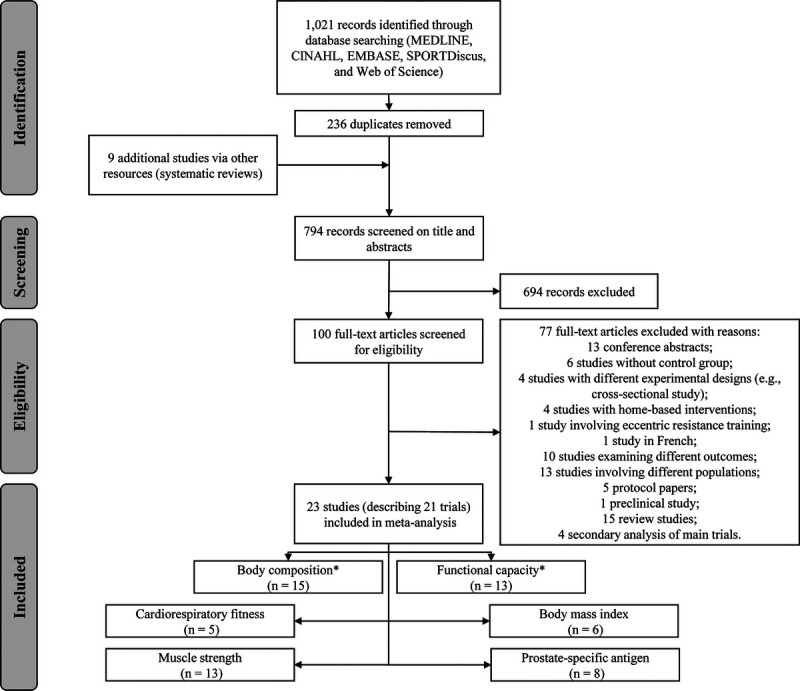
Methods: Using PRISMA guidelines, MEDLINE, CINAHL, EMBASE, SPORTDiscus, and Web of Science databases were searched. Eligible randomized controlled trials examined prostate cancer patients undertaking resistance-based exercise programs during or after treatment. Meta-analysis was undertaken when more than three studies were included. Associations between mean differences and exercise components were tested by univariate and multivariate meta-regression analysis.
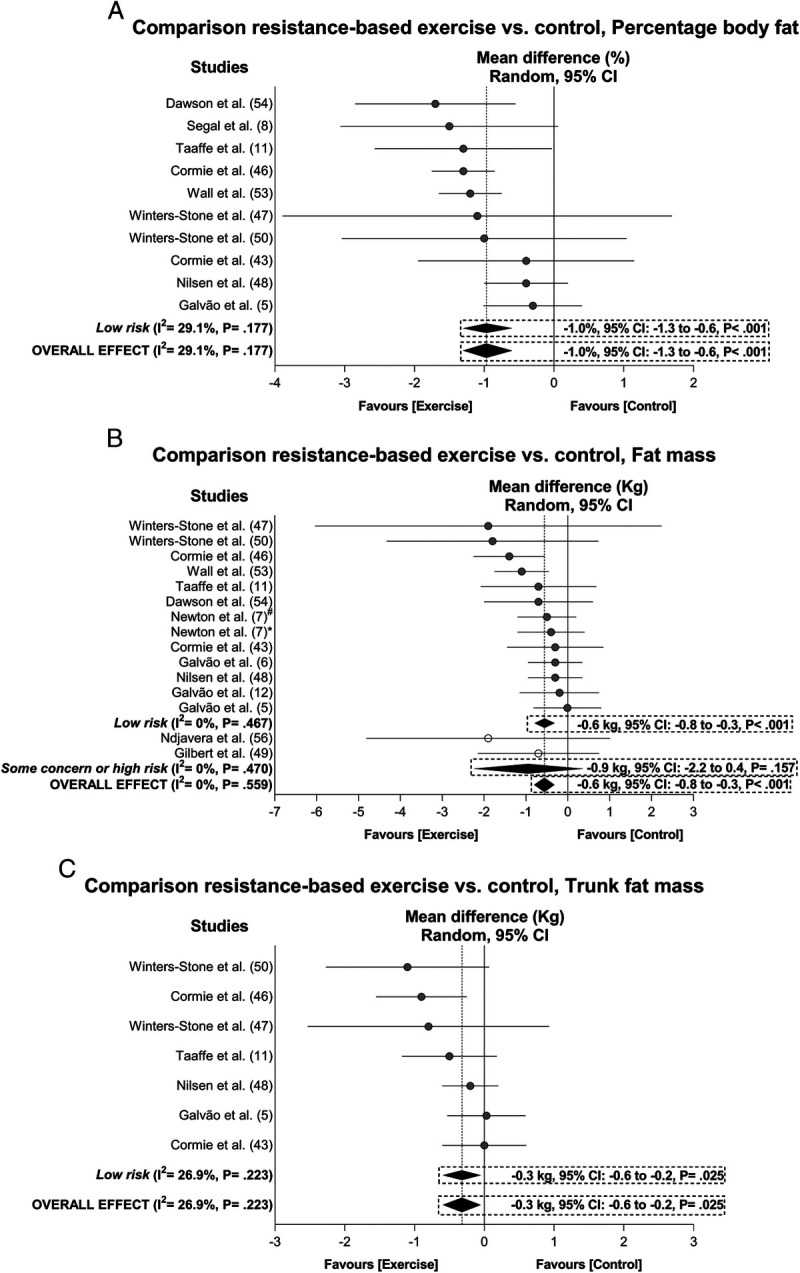
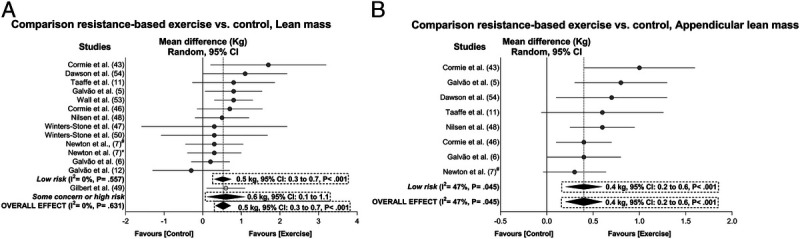
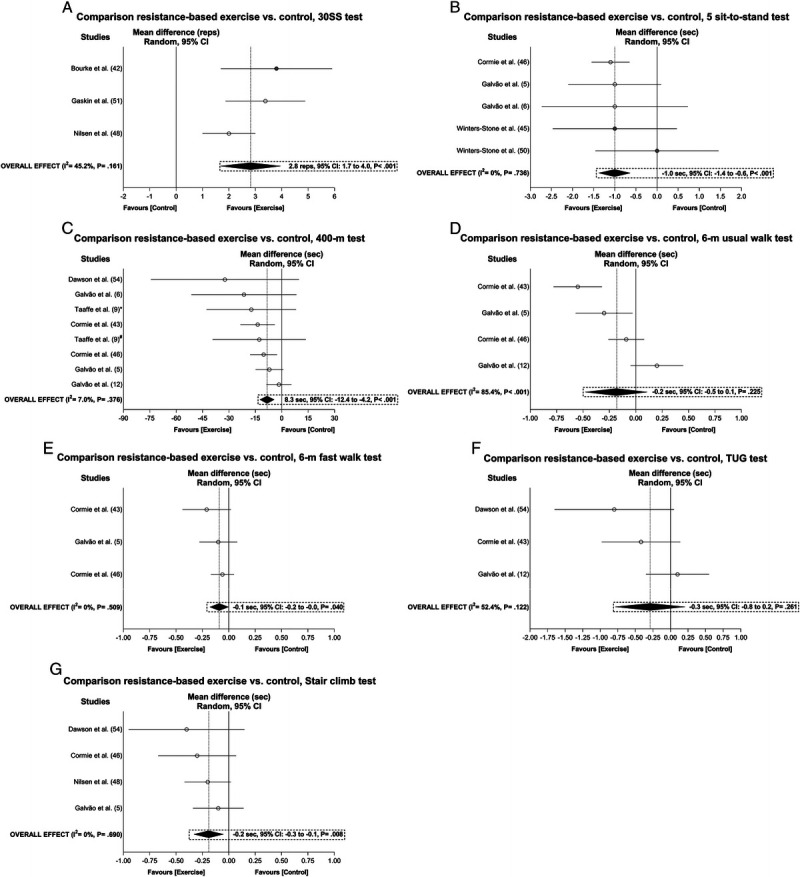
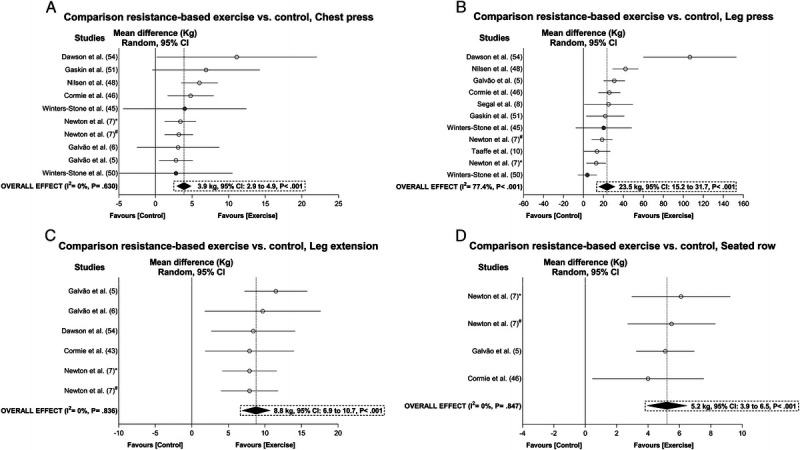
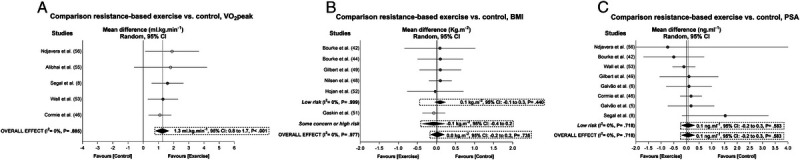
Results: Twenty-three articles describing 21 trials and involving 1748 prostate cancer patients were included. Exercise improved fat mass (-1% in body fat and -0.6 kg in fat mass), lean mass (~0.5 kg in lean and appendicular lean mass), functional capacity (i.e., chair rise, 400-m test, 6-m fast walk, and stair climb tests), and fitness outcomes (i.e., V̇O2peak and muscle strength) (P = 0.040-<0.001) with no change in body mass index or prostate-specific antigen (P = 0.440-0.735). Meta-regression indicated no association between exercise type, resistance training duration, weekly volume and intensity, and primary outcomes (P = 0.075-0.965). There was a significant association between exercise intensity and chest press muscle strength (favoring moderate intensity, P = 0.012), but not in other secondary outcomes.
Conclusion: In untrained older men with prostate cancer initiating an exercise program, lower volume at moderate to high intensity is as effective as higher volume resistance training for enhancing body composition, functional capacity, and muscle strength in the short term. A low exercise dosage may help reduce barriers to exercise and enhance adherence.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American College of Sports Medicine.
Figures
References
-
- Schmitz KH Courneya KS Matthews C, et al. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc. 2010;42(7):1409–26. - PubMed
-
- Galvão DA, Newton RU, Taaffe DR, Spry N. Can exercise ameliorate the increased risk of cardiovascular disease and diabetes associated with ADT? Nat Clin Pract Urol. 2008;5(6):306–7. - PubMed
-
- Galvão DA, Taaffe DR, Spry N, Joseph D, Newton RU. Combined resistance and aerobic exercise program reverses muscle loss in men undergoing androgen suppression therapy for prostate cancer without bone metastases: a randomized controlled trial. J Clin Oncol. 2010;28(2):340–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
