

Type 2 diabetes and reduced exercise tolerance: a review of the literature through an integrated physiology approach
- PMID: 32891175
- PMCID: PMC7487838
- DOI: 10.1186/s12933-020-01109-1
Type 2 diabetes and reduced exercise tolerance: a review of the literature through an integrated physiology approach
Abstract
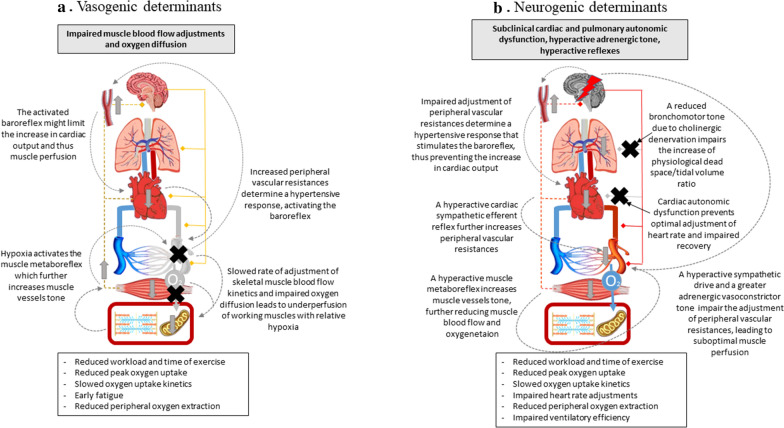
The association between type 2 diabetes mellitus (T2DM) and heart failure (HF) is well established. Early in the course of the diabetic disease, some degree of impaired exercise capacity (a powerful marker of health status with prognostic value) can be frequently highlighted in otherwise asymptomatic T2DM subjects. However, the literature is quite heterogeneous, and the underlying pathophysiologic mechanisms are far from clear. Imaging-cardiopulmonary exercise testing (CPET) is a non-invasive, provocative test providing a multi-variable assessment of pulmonary, cardiovascular, muscular, and cellular oxidative systems during exercise, capable of offering unique integrated pathophysiological information. With this review we aimed at defying the cardiorespiratory alterations revealed through imaging-CPET that appear specific of T2DM subjects without overt cardiovascular or pulmonary disease. In synthesis, there is compelling evidence indicating a reduction of peak workload, peak oxygen assumption, oxygen pulse, as well as ventilatory efficiency. On the contrary, evidence remains inconclusive about reduced peripheral oxygen extraction, impaired heart rate adjustment, and lower anaerobic threshold, compared to non-diabetic subjects. Based on the multiparametric evaluation provided by imaging-CPET, a dissection and a hierarchy of the underlying mechanisms can be obtained. Here we propose four possible integrated pathophysiological mechanisms, namely myocardiogenic, myogenic, vasculogenic and neurogenic. While each hypothesis alone can potentially explain the majority of the CPET alterations observed, seemingly different combinations exist in any given subject. Finally, a discussion on the effects -and on the physiological mechanisms-of physical activity and exercise training on oxygen uptake in T2DM subjects is also offered. The understanding of the early alterations in the cardiopulmonary response that are specific of T2DM would allow the early identification of those at a higher risk of developing HF and possibly help to understand the pathophysiological link between T2DM and HF.
Keywords: Aerobic capacity; Autonomic dysfunction; Cardiopulmonary exercise test; Diabetic cardiomyopathy; Diabetic complications; Diabetic lung; Diabetic myopathy; Exercise physiology; Exercise tolerance; Exercise training; Physical exercise; Type 2 diabetes mellitus.
Conflict of interest statement
The authors have no conflict of interest to declare.
Figures


References
-
- Lehrke M, Marx N. Diabetes mellitus and heart failure. Am J Cardiol. 2017;120(1S):S37–S47. - PubMed
-
- Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH, Jr, Wilson JR. Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation. 1991;83(3):778–786. - PubMed
-
- Blair SN, Kohl HW, Paffenbarger RS, Clark DG, Cooper KH, Gibbons LW. Physical fitness and all-cause mortality. A prospective study of healthy men and women. JAMA. 1989;262(17):2395–2401. - PubMed
-
- Nauman J, Nes BM, Lavie CJ, Jackson AS, Sui X, Coombes JS, Blair SN, Wisloff U. Prediction of cardiovascular mortality by estimated cardiorespiratory fitness independent of traditional risk factors: the HUNT study. Mayo Clin Proc. 2017;92(2):218–227. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
