

Restrictive transfusion strategy for critically injured patients (RESTRIC) trial: a study protocol for a cluster-randomised, crossover non-inferiority trial
- PMID: 32895281
- PMCID: PMC7478023
- DOI: 10.1136/bmjopen-2020-037238
Restrictive transfusion strategy for critically injured patients (RESTRIC) trial: a study protocol for a cluster-randomised, crossover non-inferiority trial
Abstract
Introduction: Resuscitation using blood products is critical during the acute postinjury period. However, the optimal target haemoglobin (Hb) levels have not been adequately investigated. With the restrictive transfusion strategy for critically injured patients (RESTRIC) trial, we aim to compare the restrictive and liberal red blood cell (RBC) transfusion strategies.
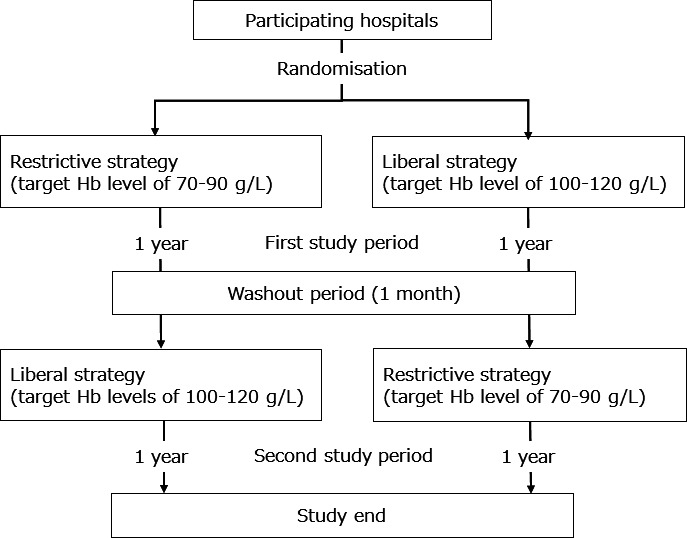
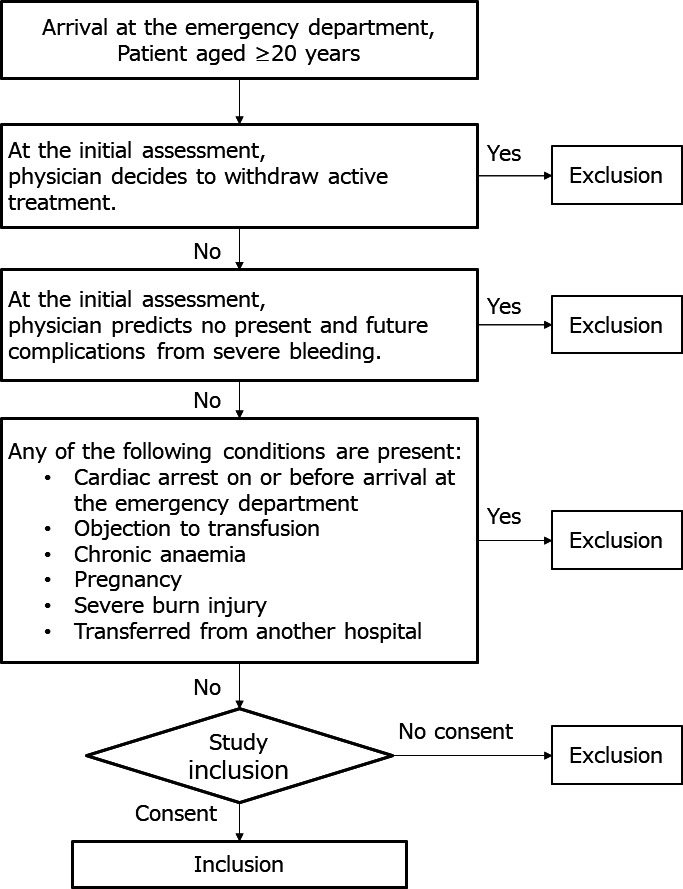
Methods and analysis: This is a cluster-randomised, crossover, non-inferiority trial of patients with severe trauma at 22 hospitals that have been randomised in a 1:1 ratio based on the use of a restrictive or liberal transfusion strategy with target Hb levels of 70-90 or 100-120 g/L, respectively, during the first year. Subsequently, after 1-month washout period, another transfusion strategy will be applied for an additional year. RBC transfusion requirements are usually unclear on arrival at the emergency department. Therefore, patients with severe bleeding, which could lead to haemorrhagic shock, will be included in the trial based on the attending physician's judgement. Each RBC transfusion strategy will be applied until 7 days postadmission to the hospital or discharge from the intensive care unit. The outcomes measured will include the 28-day survival rate after arrival at the emergency department (primary), the cumulative amount of blood transfused, event-free days and frequency of transfusion-associated lung injury and organ failure (secondary). Demonstration of the non-inferiority of restrictive transfusion will emphasise its clinical advantages.
Ethics and dissemination: The trial will be performed according to the Japanese and International Ethical guidelines. It has been approved by the Ethics Committee of each participating hospital and The Japanese Association for the Surgery of Trauma (JAST). Written informed consent will be obtained from all patients or their representatives. The results of the trial will be disseminated to the participating hospitals and board-certified educational institutions of JAST, submitted to peer-reviewed journals for publication, and presented at congresses.
Trial registration number: UMIN Clinical Trials Registry; UMIN000034405. Registered 8 October 2018.
Keywords: accident & emergency medicine; blood bank & transfusion medicine; haematology; trauma management.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Johansson PI, Sørensen AM, Larsen CF, et al. . Low hemorrhage-related mortality in trauma patients in a level I trauma center employing transfusion packages and early thromboelastography-directed hemostatic resuscitation with plasma and platelets. Transfusion 2013;53:3088–99. 10.1111/trf.12214 - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
- Actions
LinkOut - more resources
Full Text Sources
Medical