

Developing a COVID-19 mortality risk prediction model when individual-level data are not available
- PMID: 32895375
- PMCID: PMC7477233
- DOI: 10.1038/s41467-020-18297-9
Developing a COVID-19 mortality risk prediction model when individual-level data are not available
Abstract
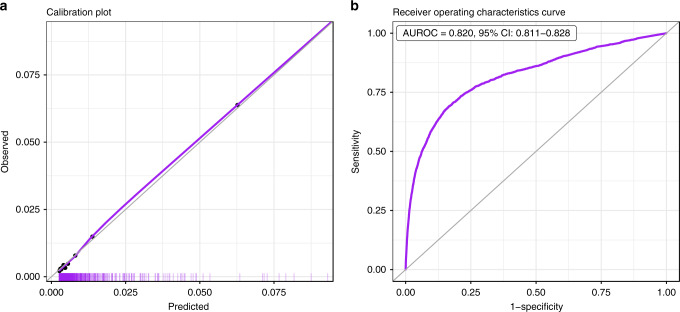
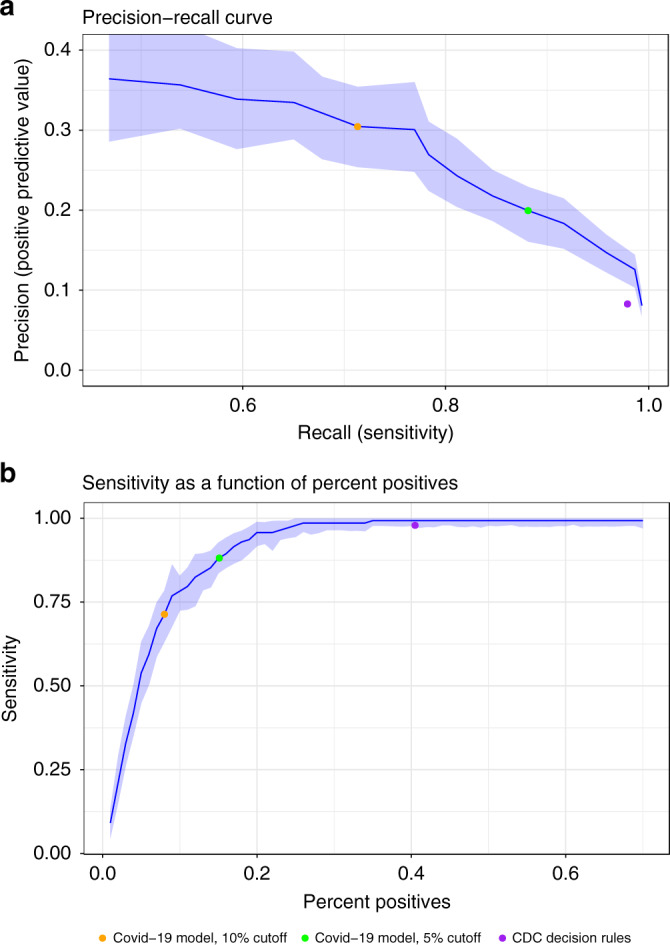
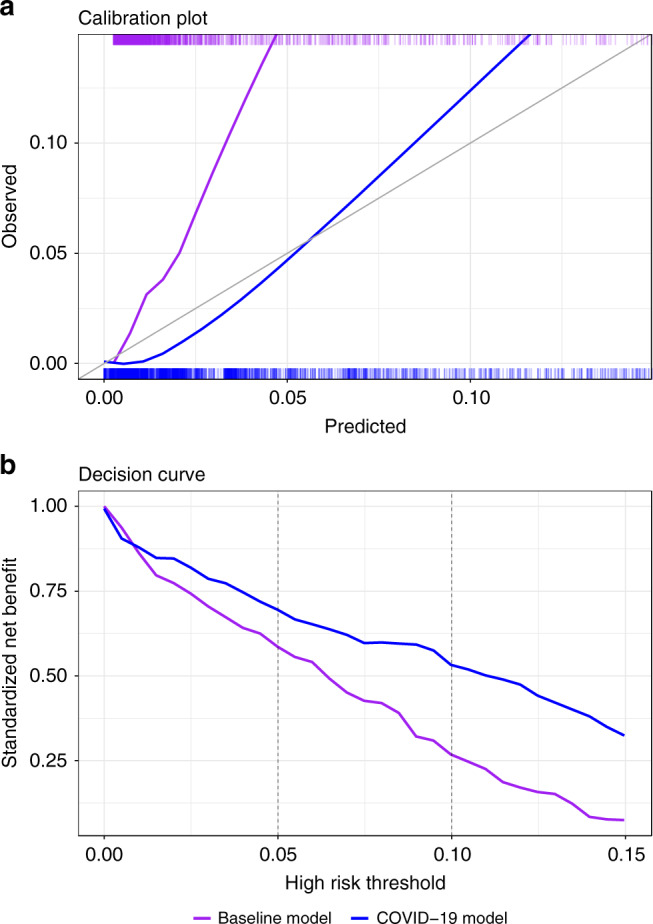
At the COVID-19 pandemic onset, when individual-level data of COVID-19 patients were not yet available, there was already a need for risk predictors to support prevention and treatment decisions. Here, we report a hybrid strategy to create such a predictor, combining the development of a baseline severe respiratory infection risk predictor and a post-processing method to calibrate the predictions to reported COVID-19 case-fatality rates. With the accumulation of a COVID-19 patient cohort, this predictor is validated to have good discrimination (area under the receiver-operating characteristics curve of 0.943) and calibration (markedly improved compared to that of the baseline predictor). At a 5% risk threshold, 15% of patients are marked as high-risk, achieving a sensitivity of 88%. We thus demonstrate that even at the onset of a pandemic, shrouded in epidemiologic fog of war, it is possible to provide a useful risk predictor, now widely used in a large healthcare organization.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Centers for Disease Control and Prevention. People Who Are at Higher Risk for Severe Illness, Vol. 2020 (Centers for Disease Control and Prevention, 2020). https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
