

Prognostic and predictive value of circulating tumor DNA during neoadjuvant chemotherapy for triple negative breast cancer
- PMID: 32895401
- PMCID: PMC7477566
- DOI: 10.1038/s41598-020-71236-y
Prognostic and predictive value of circulating tumor DNA during neoadjuvant chemotherapy for triple negative breast cancer
Abstract
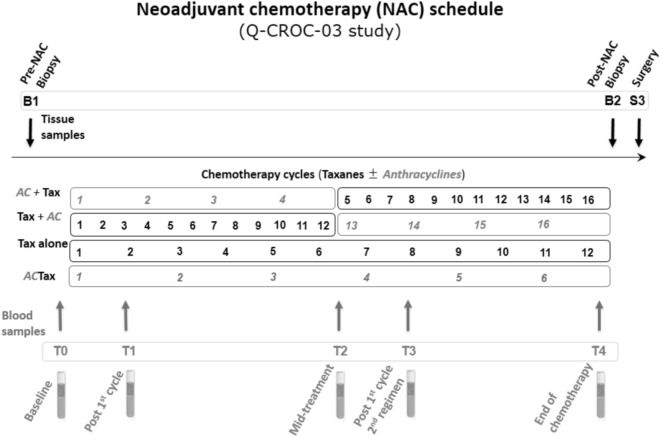
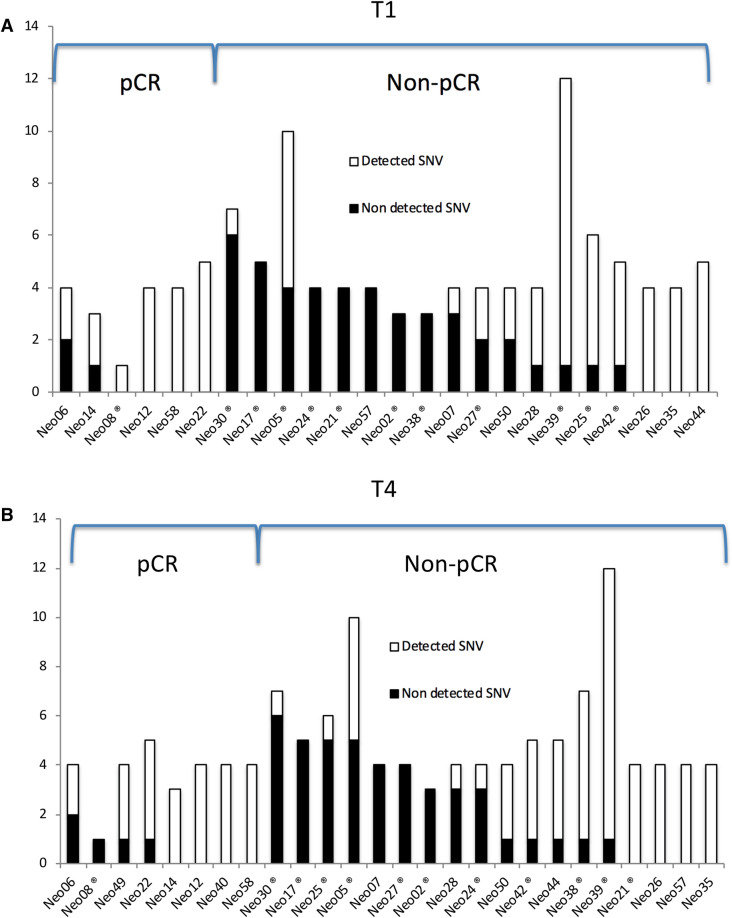
Response to neoadjuvant chemotherapy (NAC) in triple negative breast cancer (TNBC) is highly prognostic and determines whether adjuvant chemotherapy is needed if residual tumor is found at surgery. To evaluate the predictive and prognostic values of circulating tumor DNA (ctDNA) in this setting, we analyzed tumor and serial bloods from 26 TNBC patients collected prior, during, and after NAC. Individual digital droplet PCR assays were developed for 121 variants (average 5/patient) identified from tumor sequencing, enabling ctDNA detection in 96% of patients at baseline. Mutant allele frequency at baseline was associated with clinical characteristics. Levels drastically fell after one cycle of NAC, especially in patients whose tumors would go on to have a pathological complete response (pCR), but then rose significantly before surgery in patients with significant residual tumor at surgery (p = 0.0001). The detection of ctDNA early during treatment and also late at the end of NAC before surgery was strongly predictive of residual tumor at surgery, but its absence was less predictive of pCR, especially when only TP53 variants are considered. ctDNA detection at the end of neoadjuvant chemotherapy indicated significantly worse relapse-free survival (HR = 0.29 (95% CI 0.08-0.98), p = 0.046), and overall survival (HR = 0.27 95% CI 0.075-0.96), p = 0.043). Hence, individualized multi-variant ctDNA testing during and after NAC prior to surgery has prognostic and predictive value in early TNBC patients.
Conflict of interest statement
The authors declare no competing interests.
Figures



References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
