

Avelumab plus axitinib versus sunitinib in advanced renal cell carcinoma: biomarker analysis of the phase 3 JAVELIN Renal 101 trial
- PMID: 32895571
- PMCID: PMC8493486
- DOI: 10.1038/s41591-020-1044-8
Avelumab plus axitinib versus sunitinib in advanced renal cell carcinoma: biomarker analysis of the phase 3 JAVELIN Renal 101 trial
Abstract
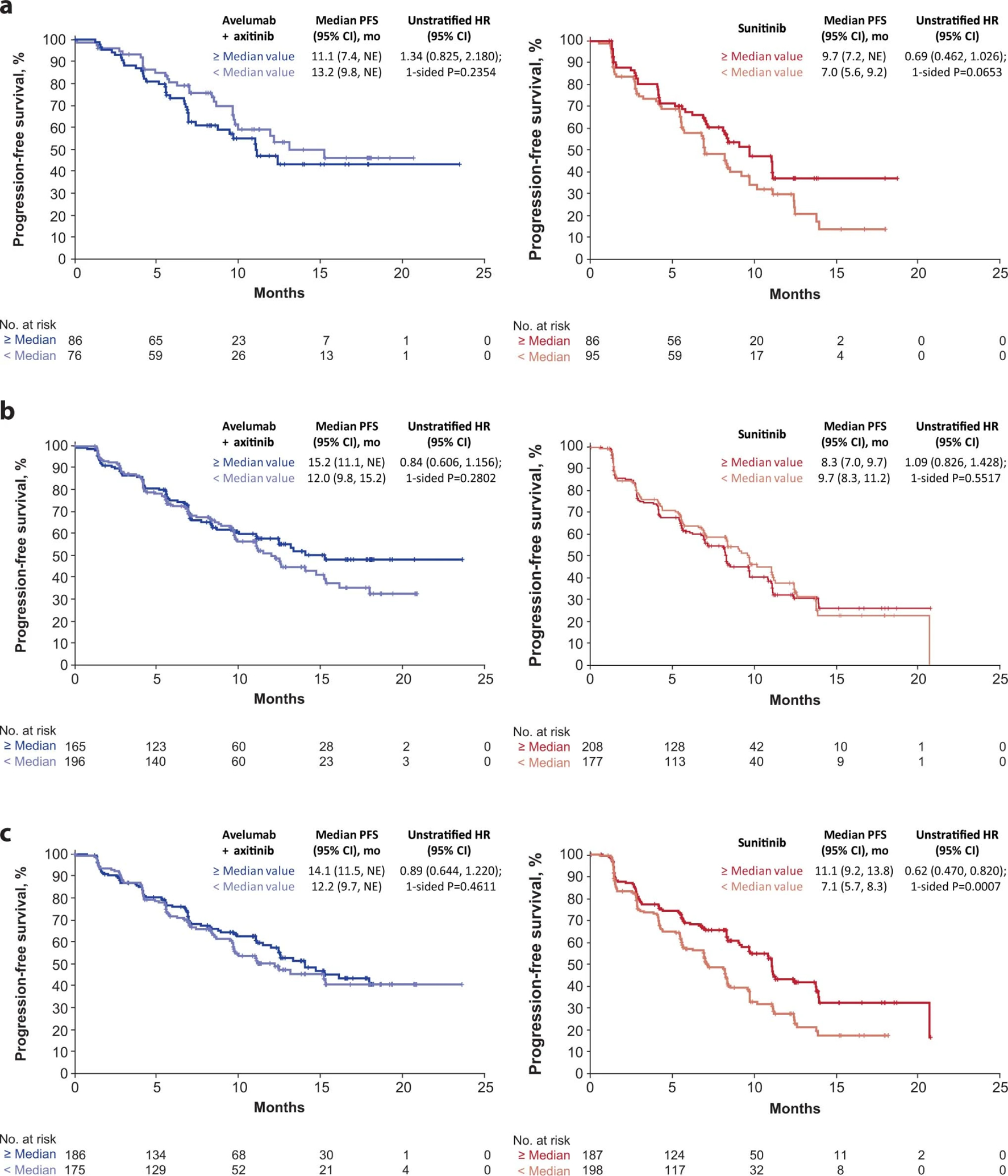
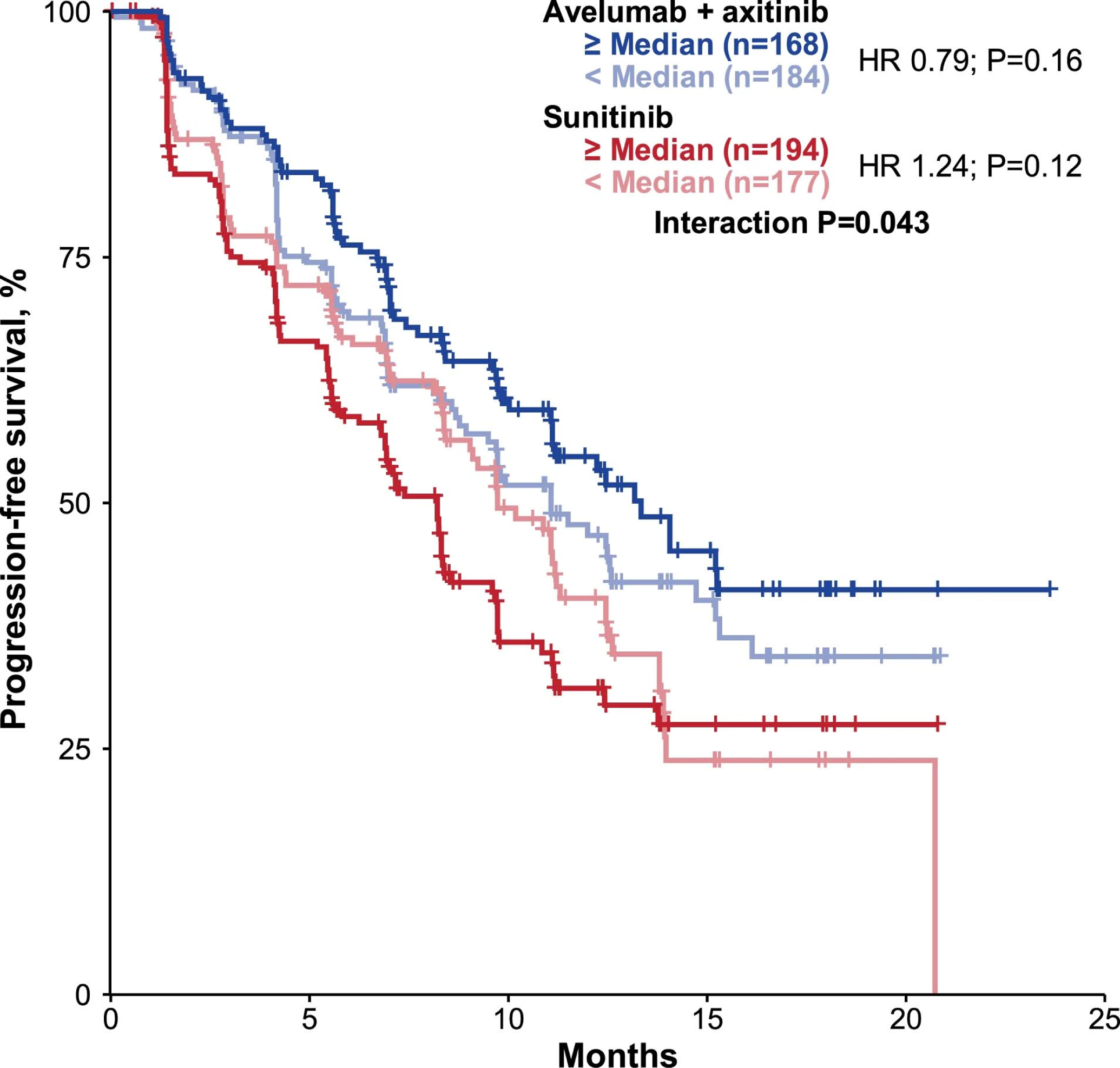
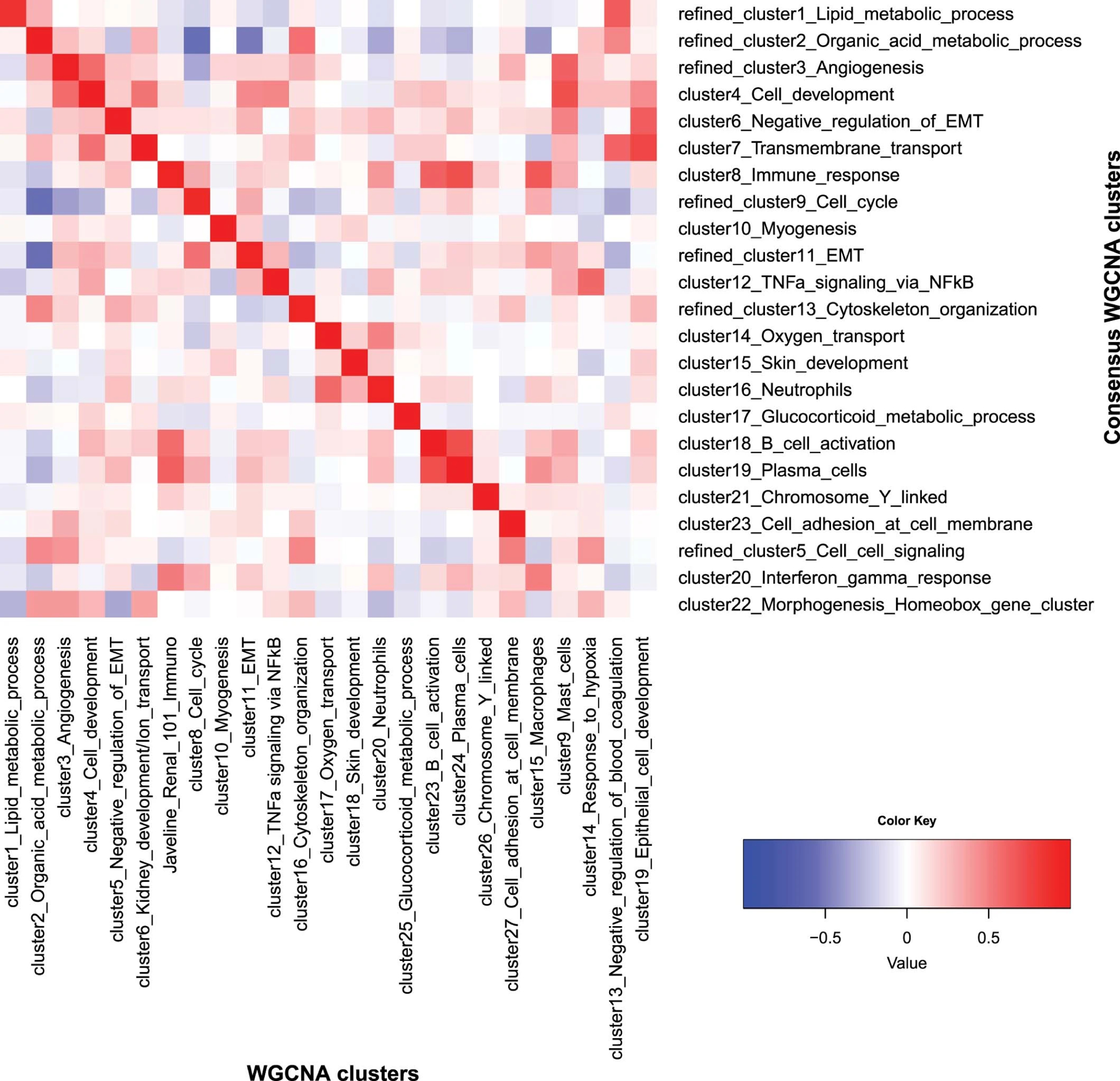
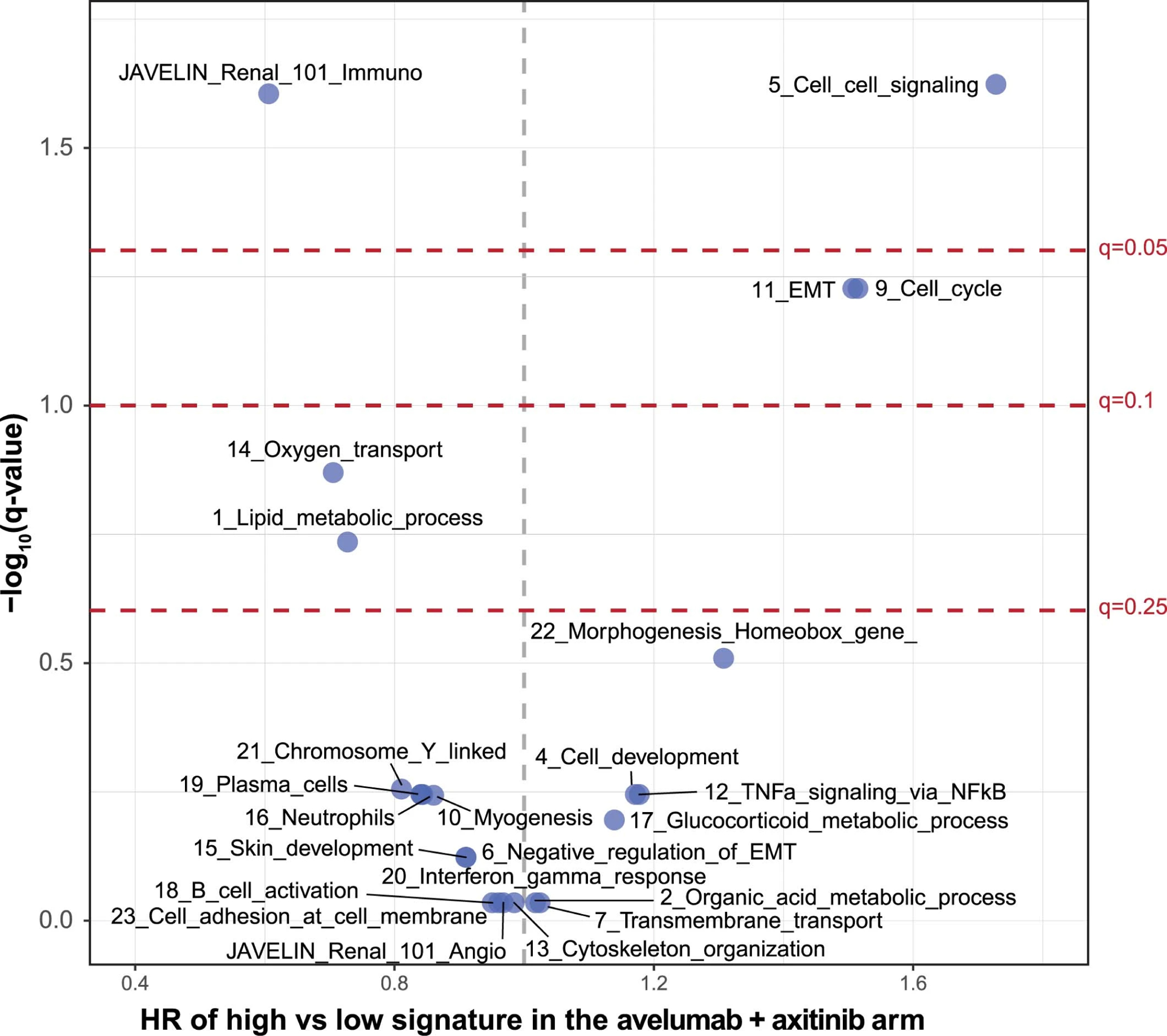
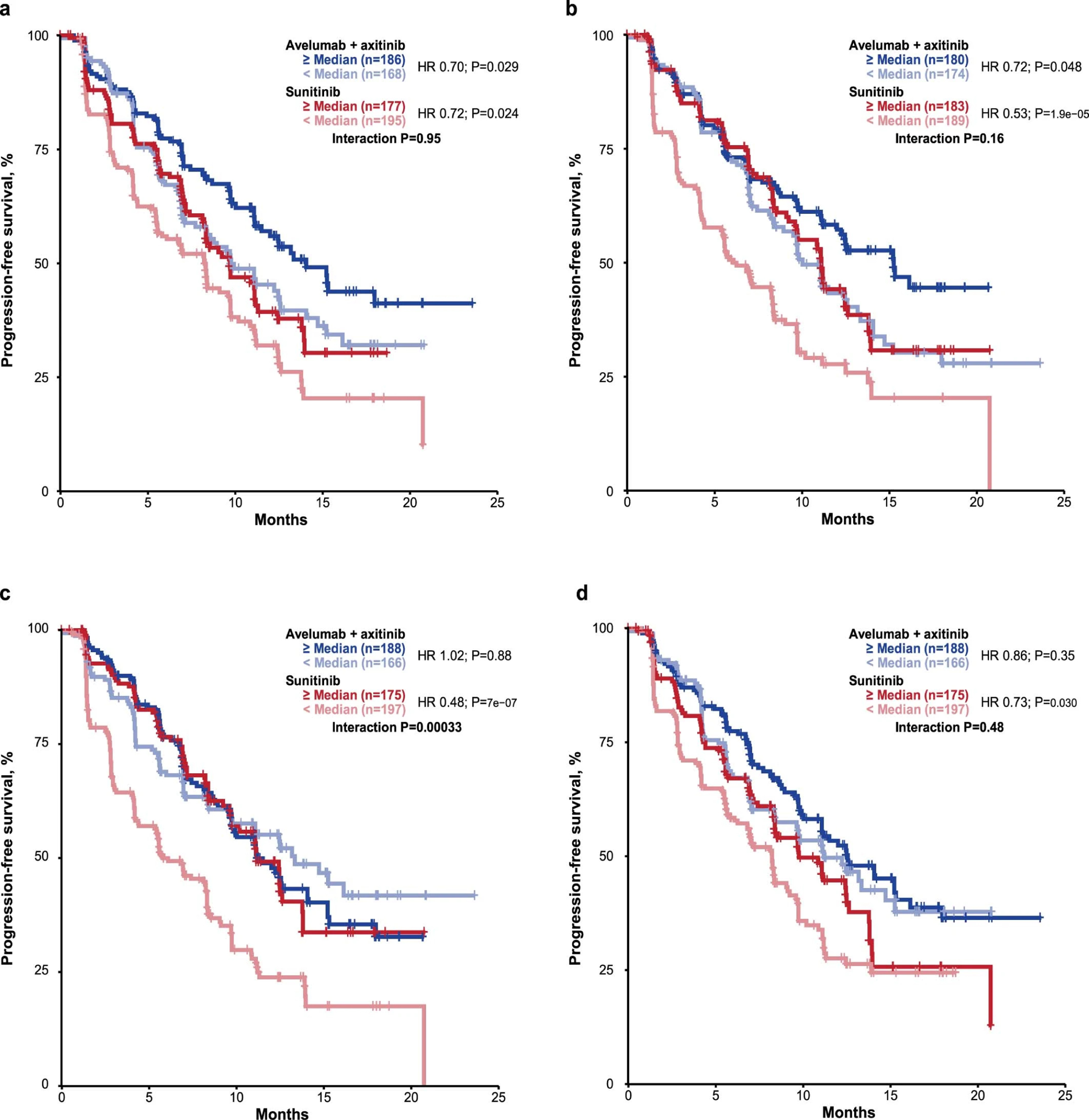
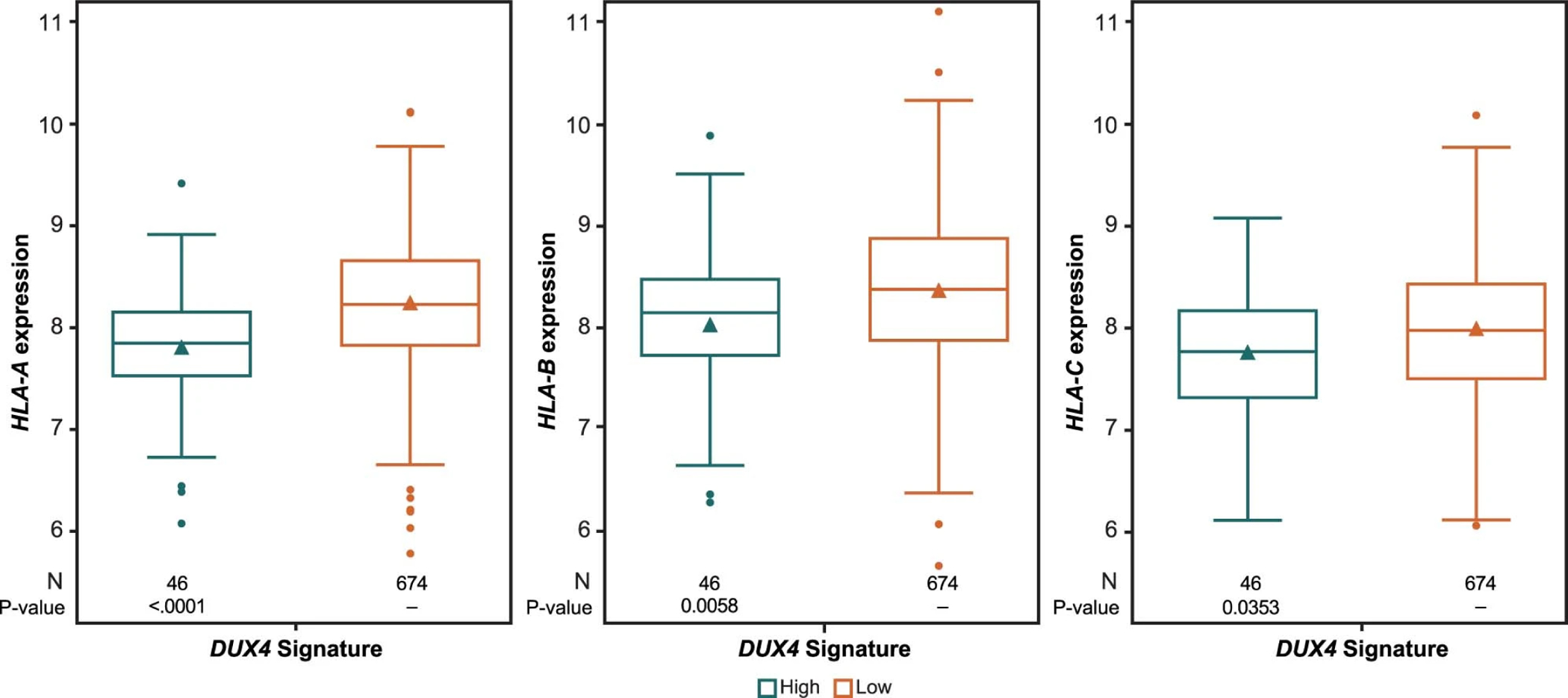
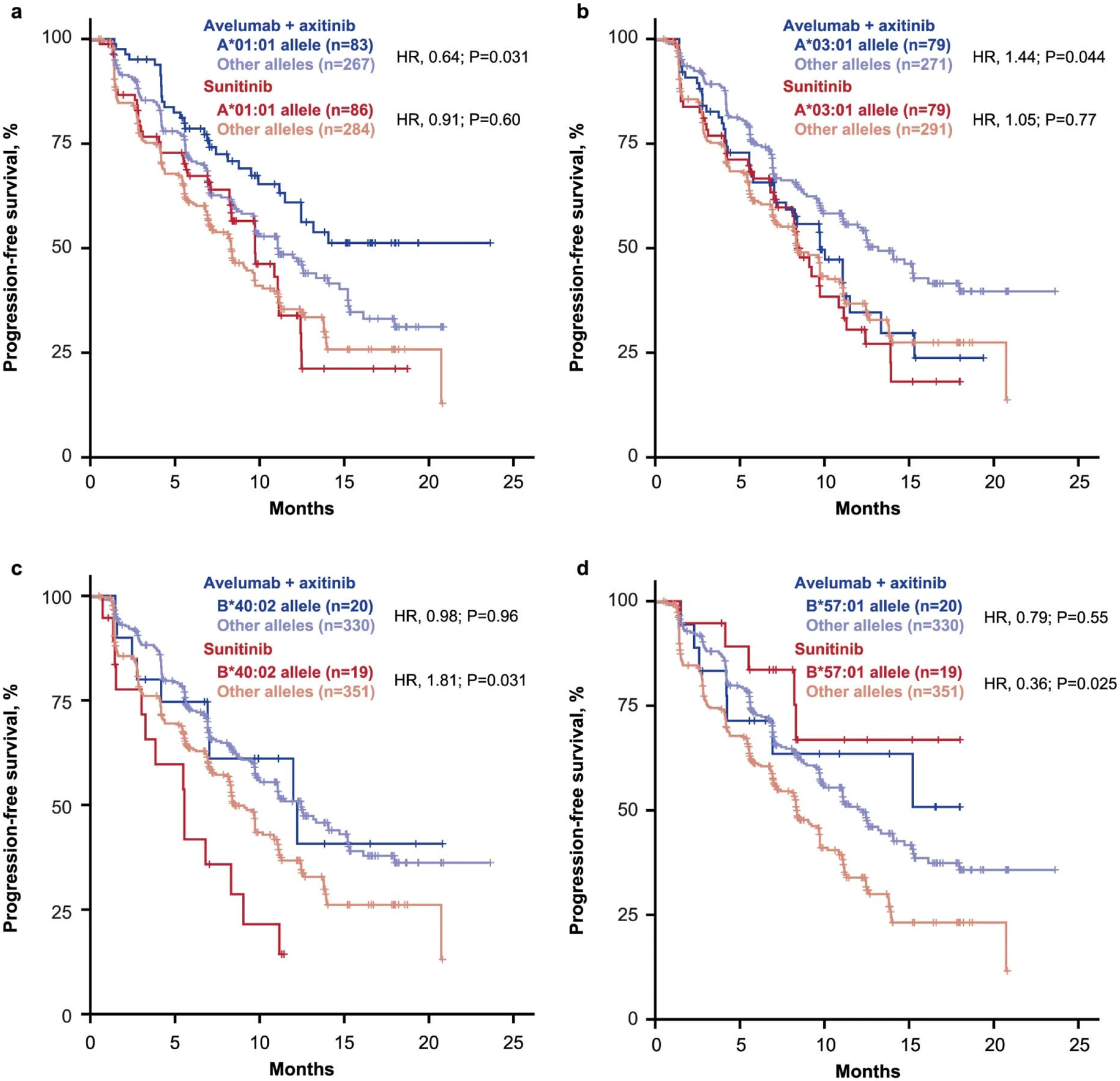
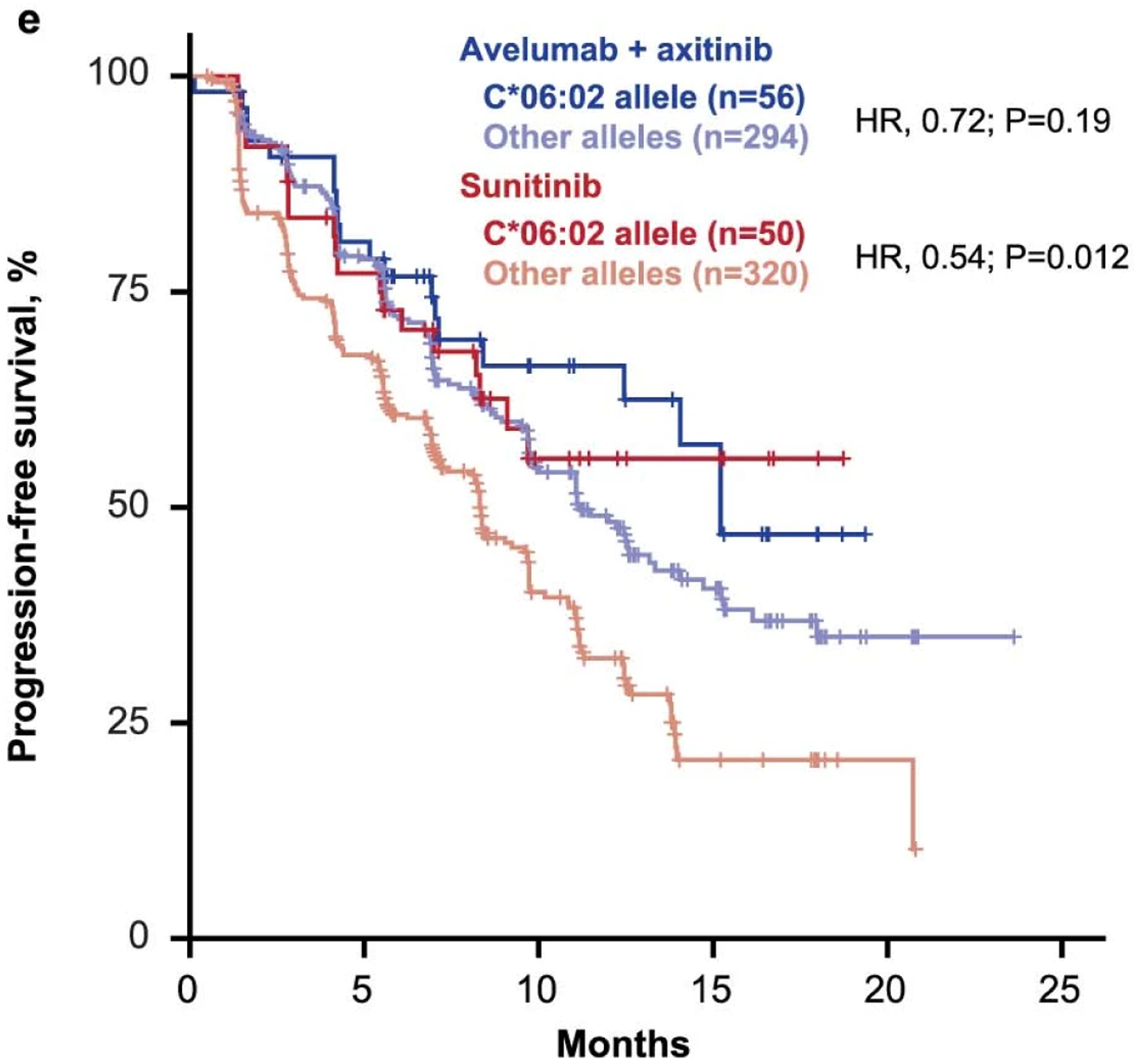
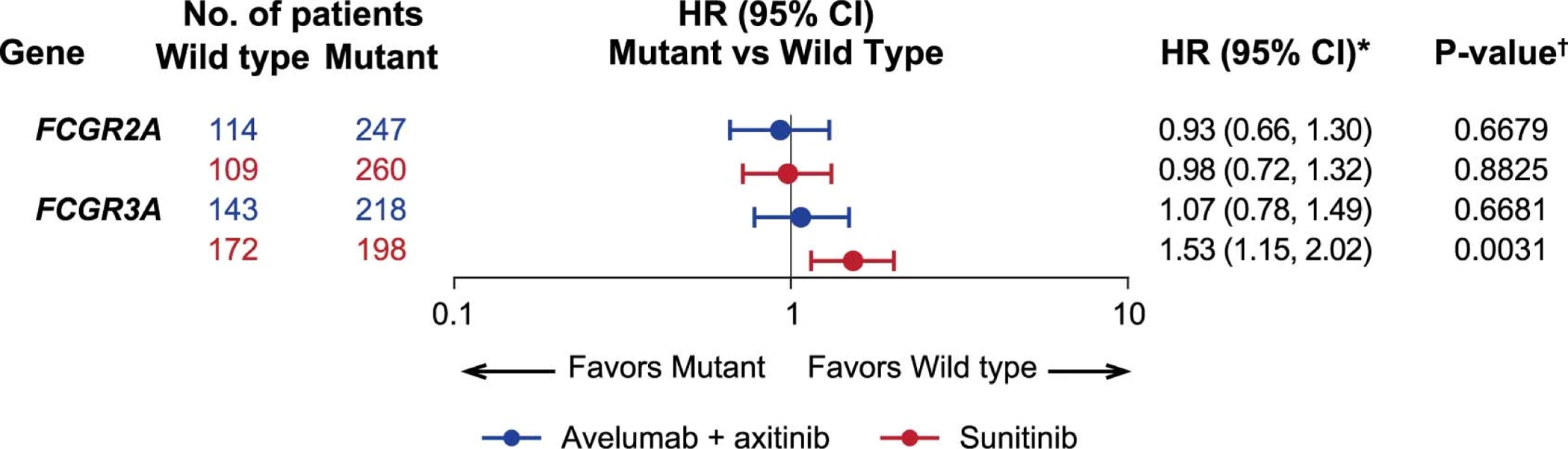
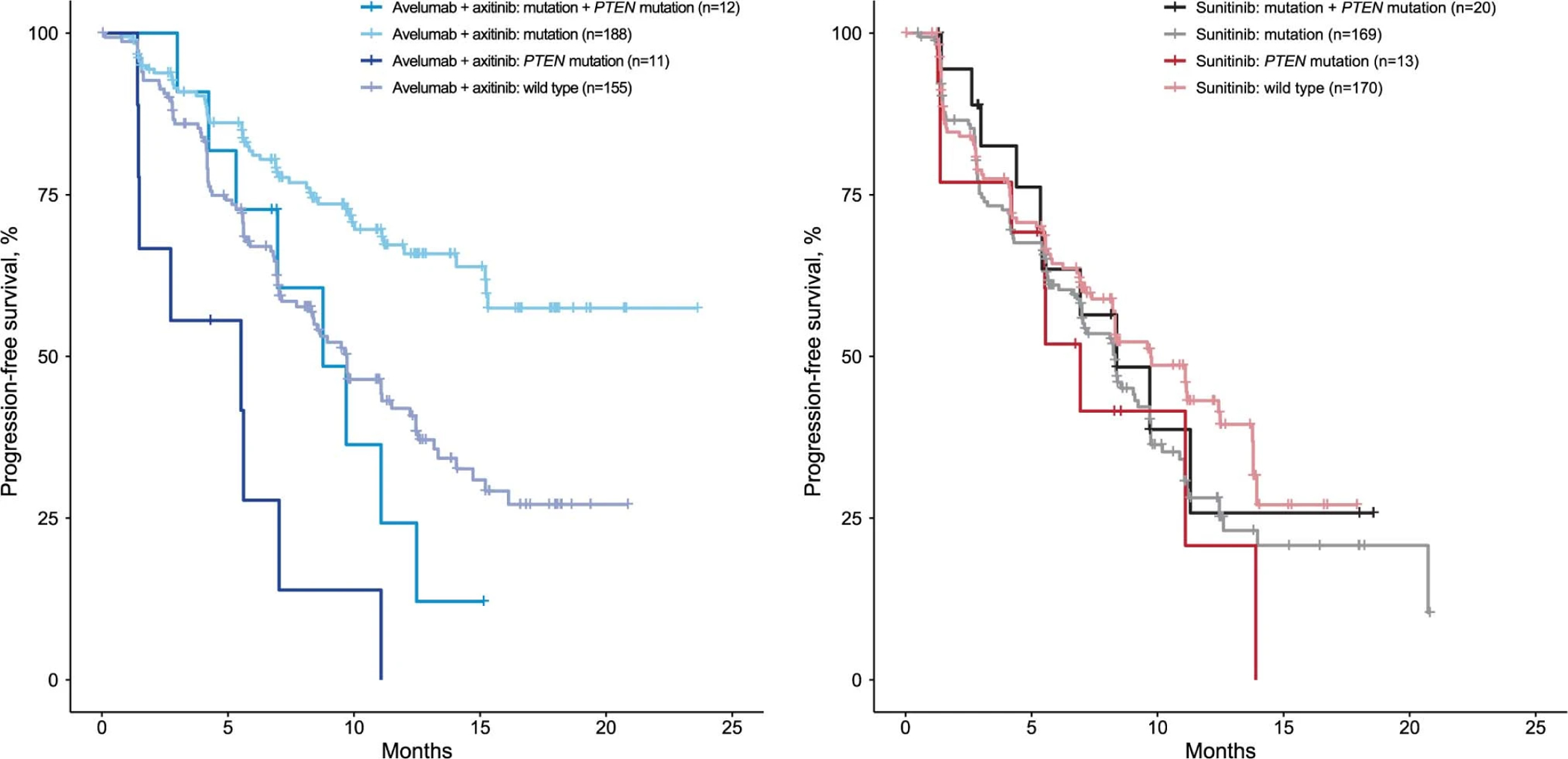
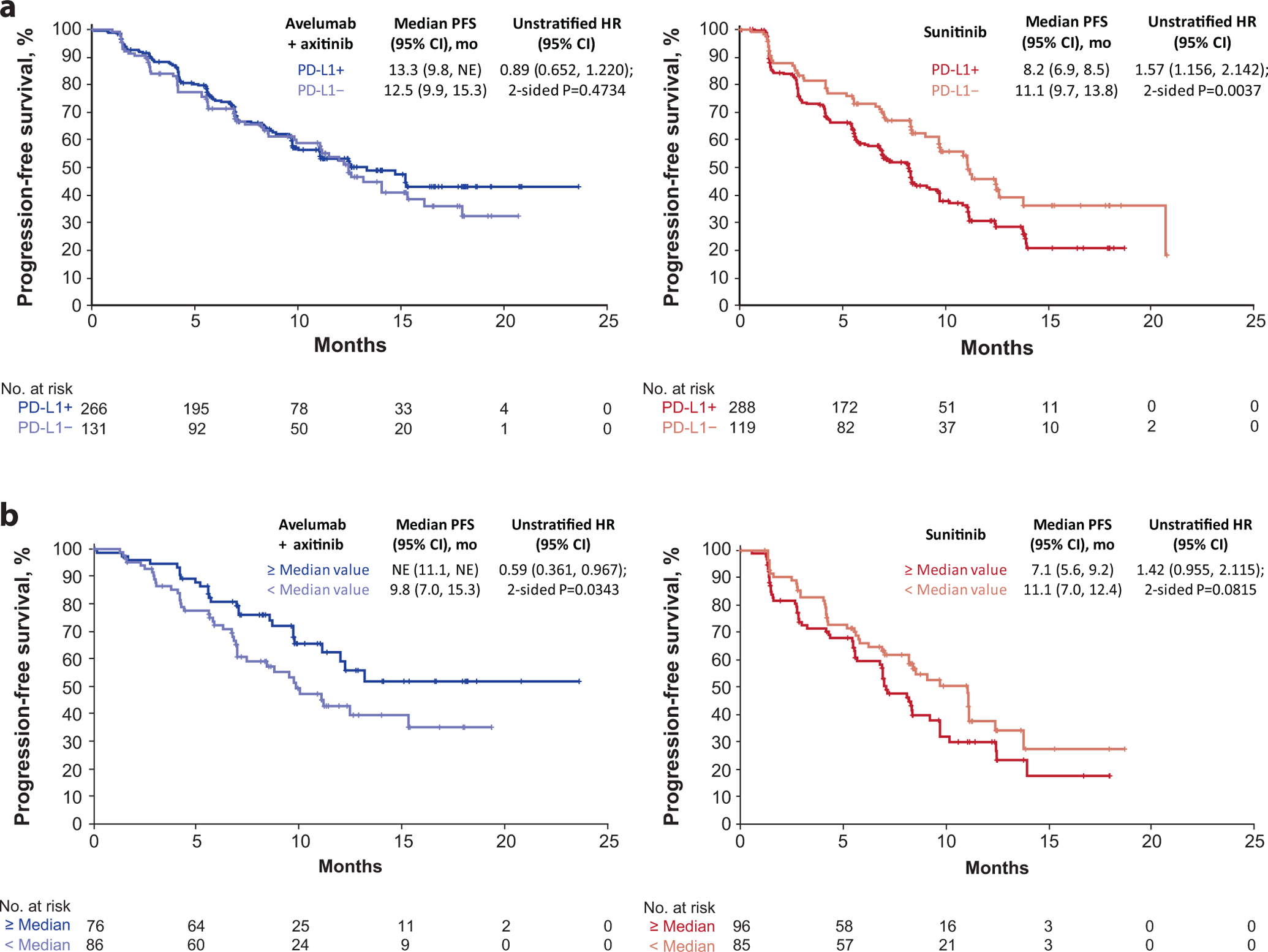
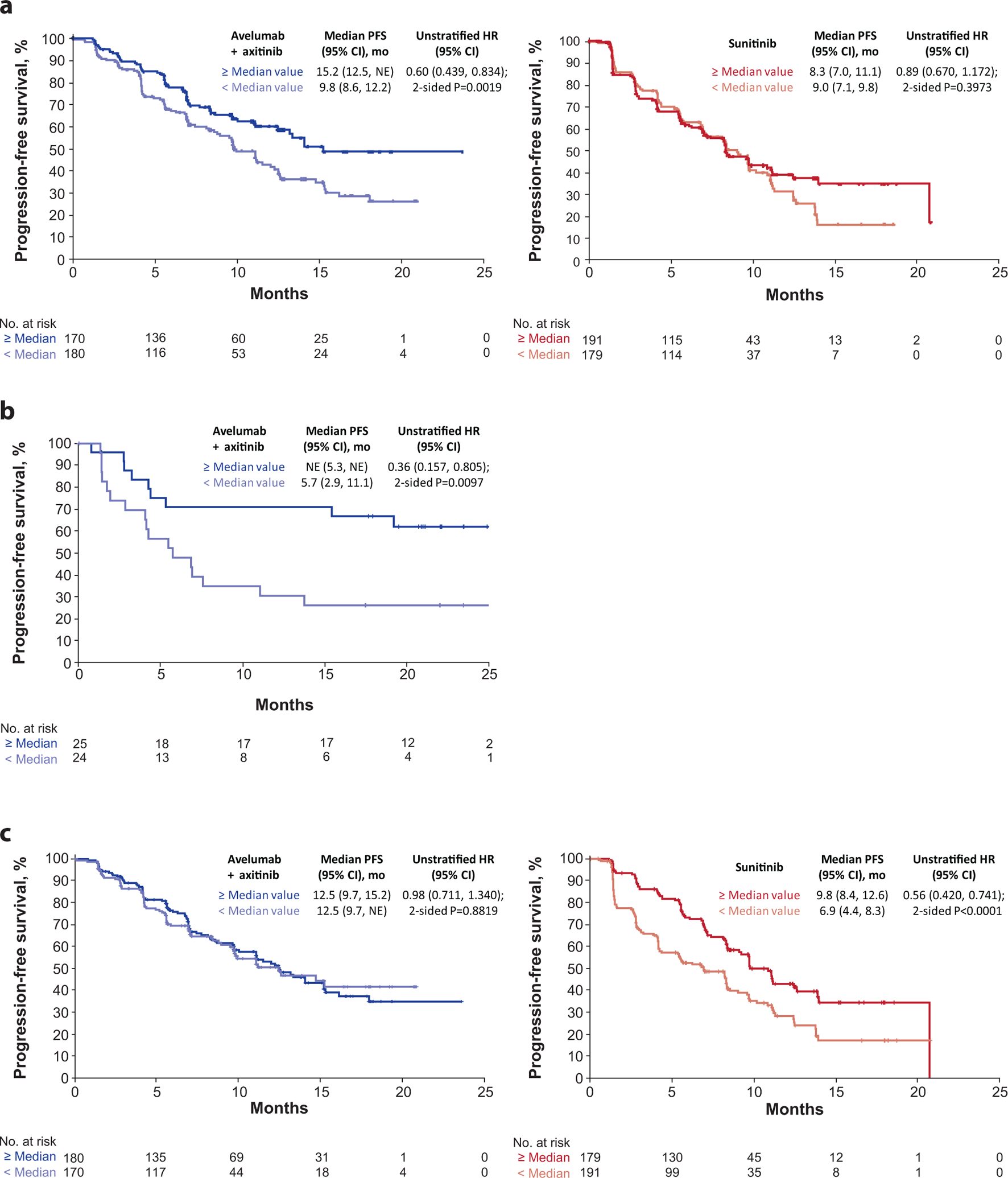
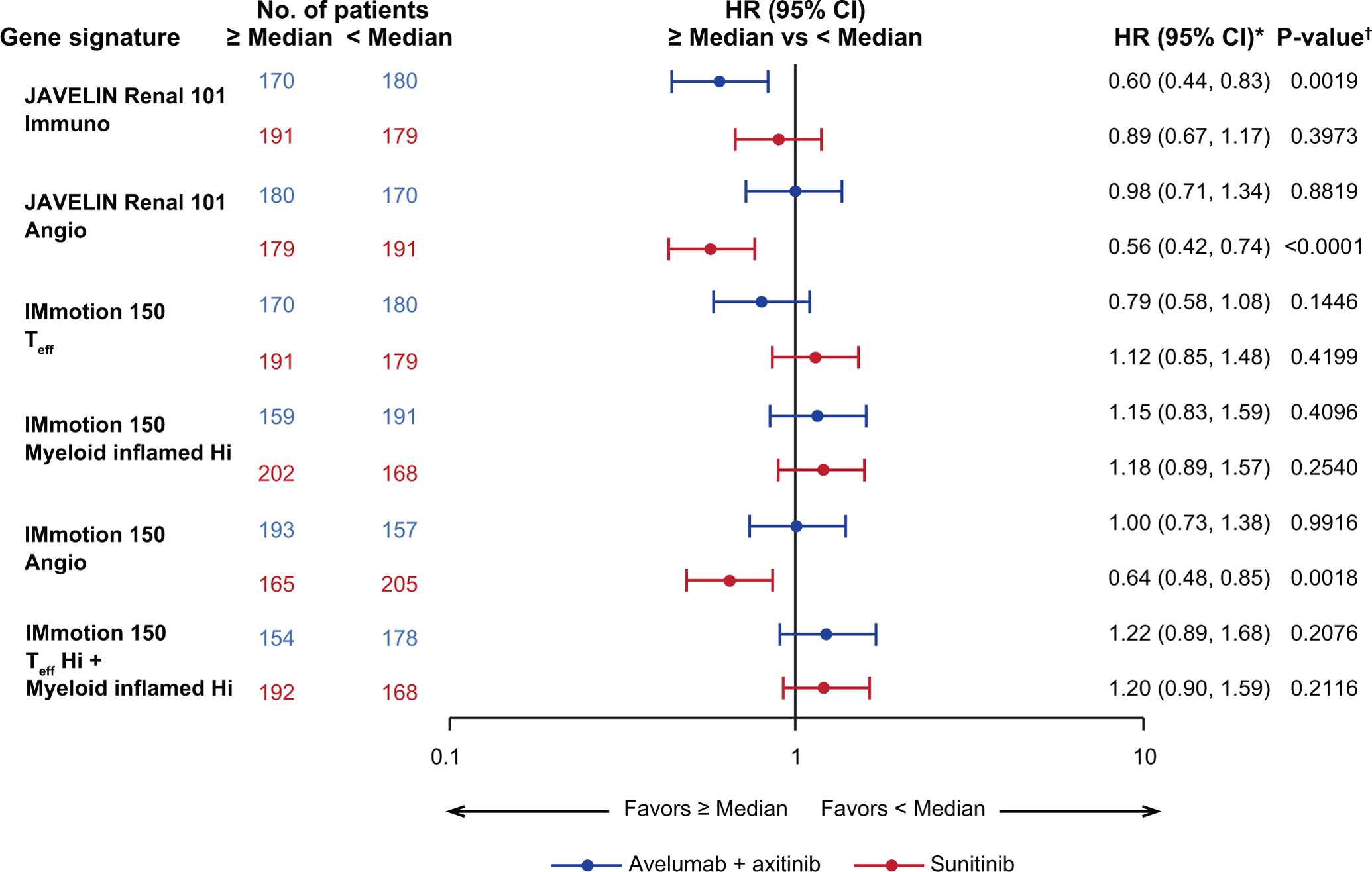
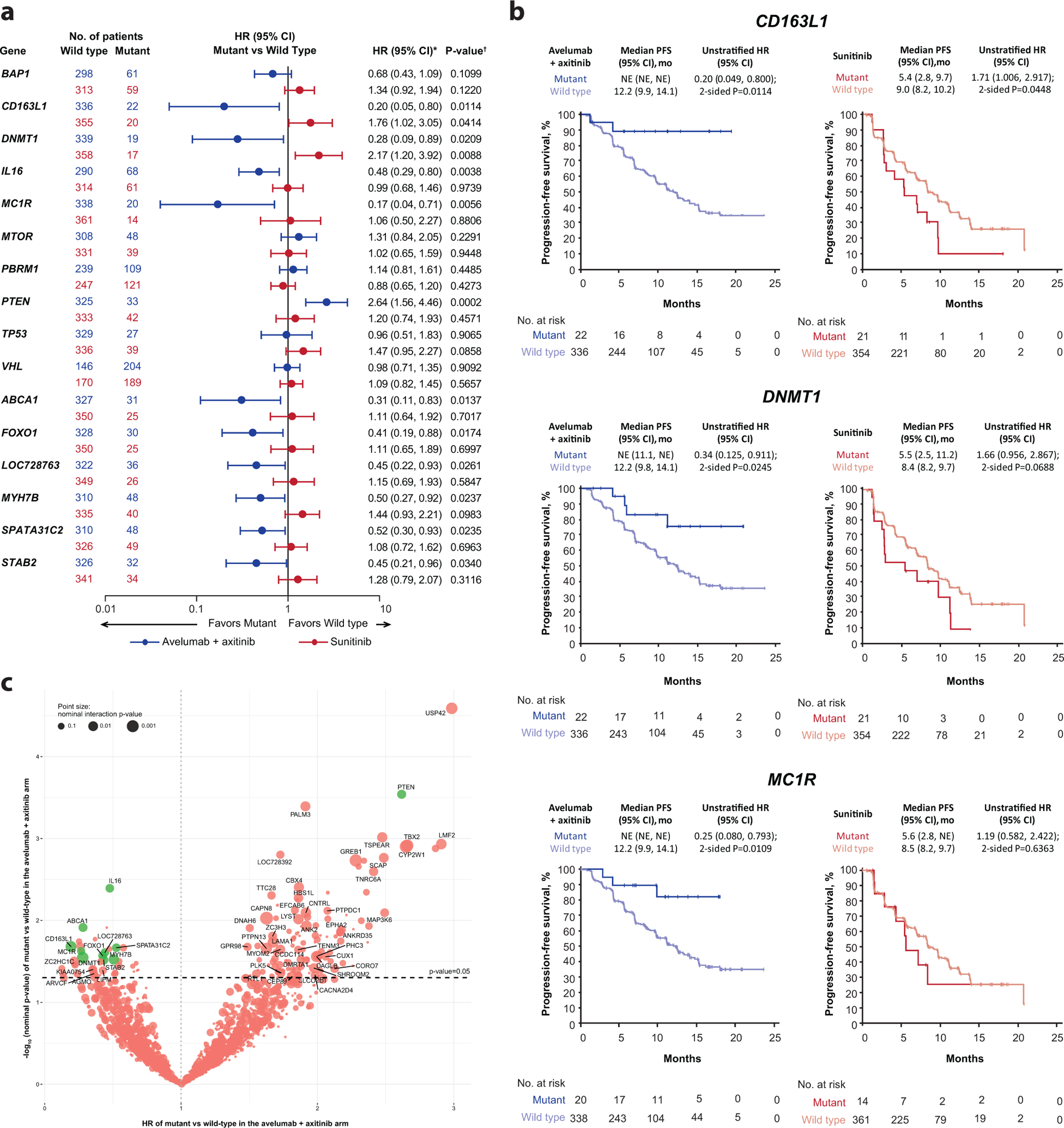
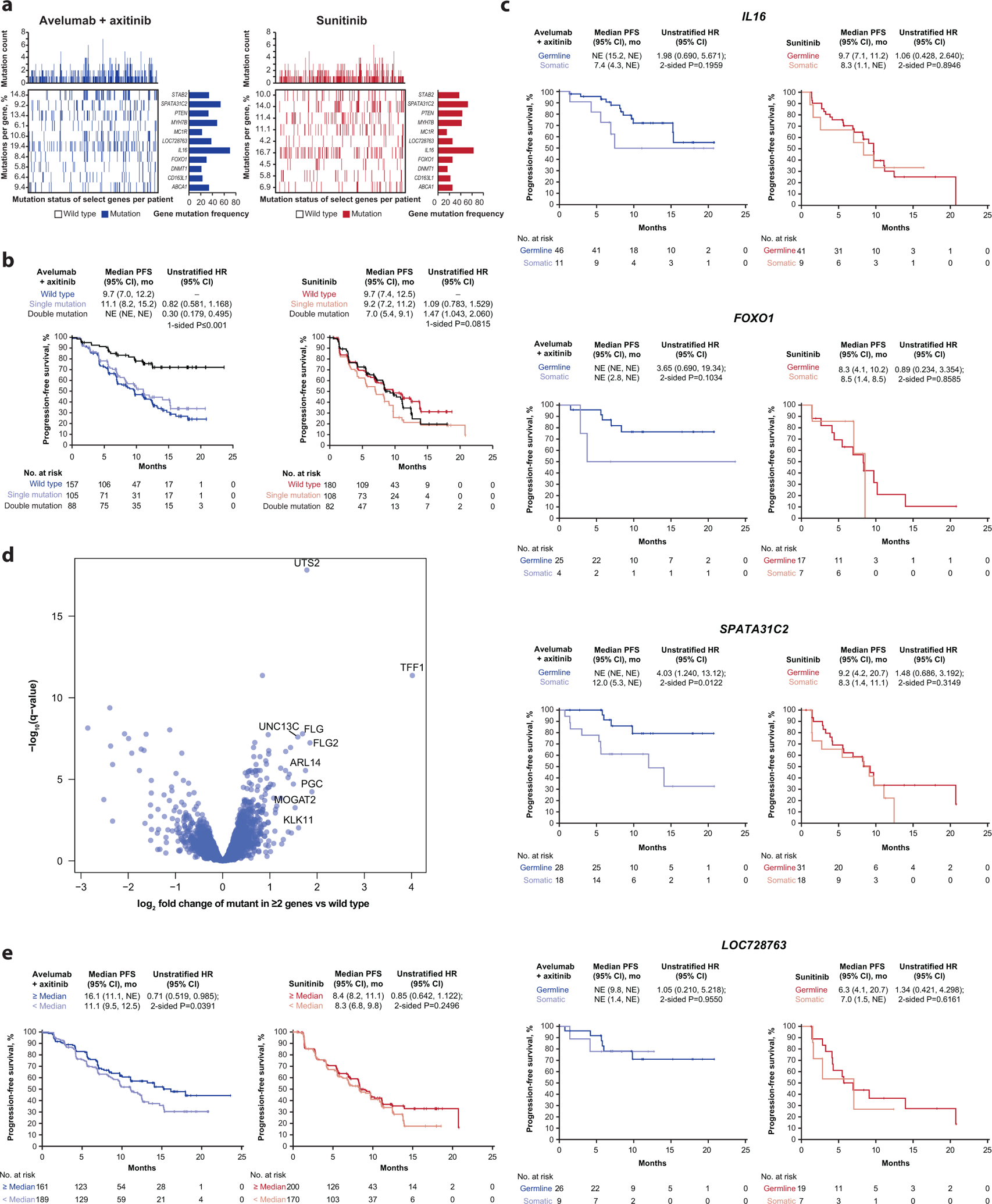
We report on molecular analyses of baseline tumor samples from the phase 3 JAVELIN Renal 101 trial (n = 886; NCT02684006 ), which demonstrated significantly prolonged progression-free survival (PFS) with first-line avelumab + axitinib versus sunitinib in advanced renal cell carcinoma (aRCC). We found that neither expression of the commonly assessed biomarker programmed cell death ligand 1 (PD-L1) nor tumor mutational burden differentiated PFS in either study arm. Similarly, the presence of FcɣR single nucleotide polymorphisms was unimpactful. We identified important biological features associated with differential PFS between the treatment arms, including new immunomodulatory and angiogenesis gene expression signatures (GESs), previously undescribed mutational profiles and their corresponding GESs, and several HLA types. These findings provide insight into the determinants of response to combined PD-1/PD-L1 and angiogenic pathway inhibition and may aid in the development of strategies for improved patient care in aRCC.
Figures
Comment in
-
Biomarkers 101 - personalizing therapy for RCC.Nat Rev Clin Oncol. 2020 Nov;17(11):653. doi: 10.1038/s41571-020-00434-4. Nat Rev Clin Oncol. 2020. PMID: 32948859 No abstract available.
-
Biomarkers 101 - personalizing therapy for RCC.Nat Rev Urol. 2020 Nov;17(11):601. doi: 10.1038/s41585-020-00380-x. Nat Rev Urol. 2020. PMID: 32968239 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
