

Genomic copy number predicts esophageal cancer years before transformation
- PMID: 32895572
- PMCID: PMC7116403
- DOI: 10.1038/s41591-020-1033-y
Genomic copy number predicts esophageal cancer years before transformation
Abstract
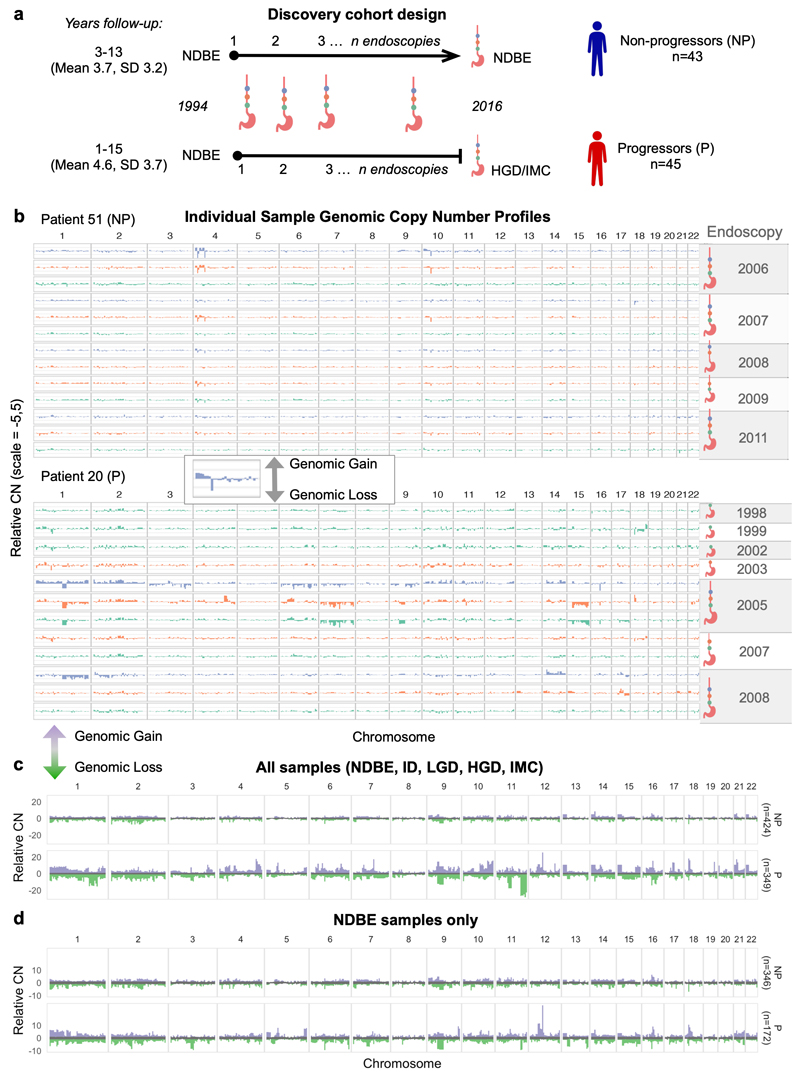
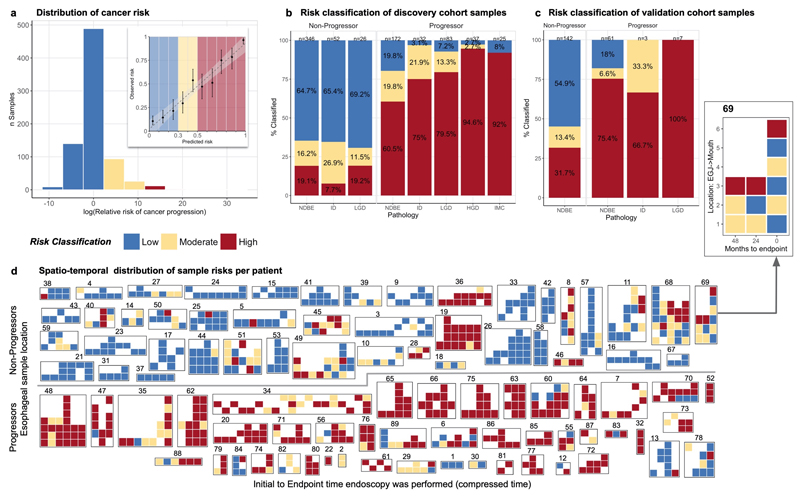
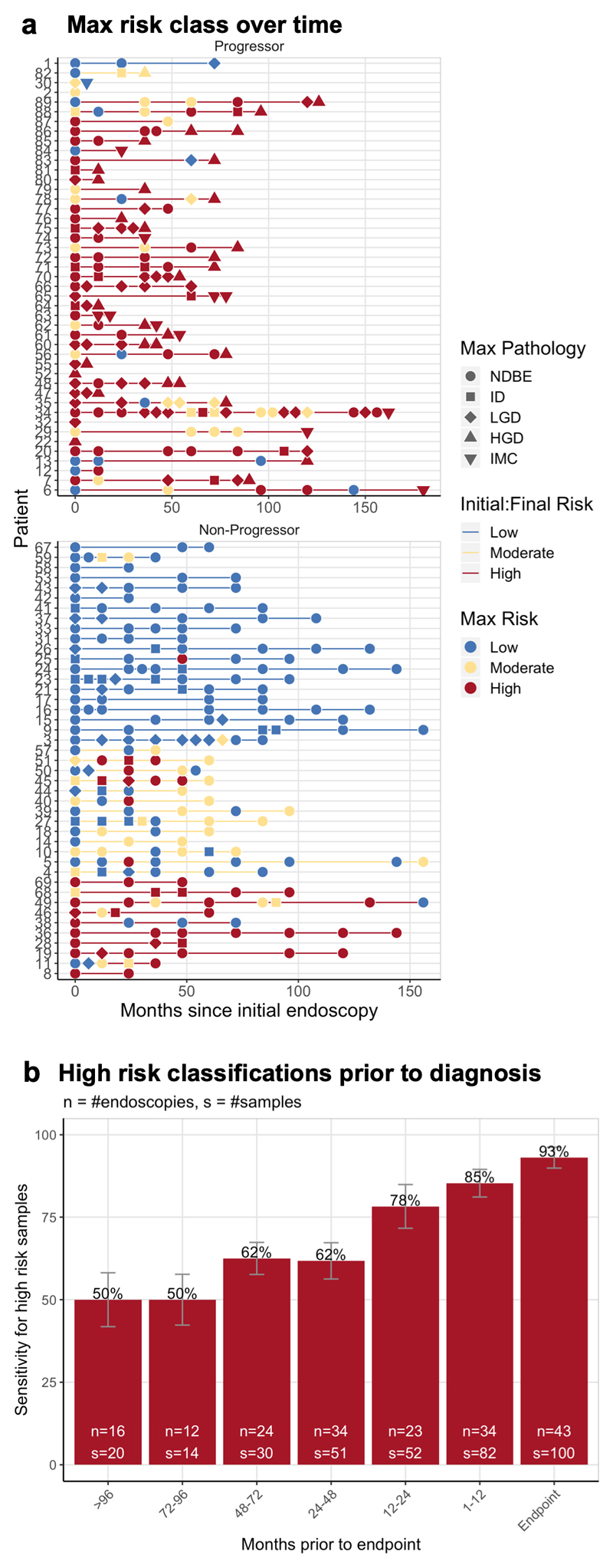
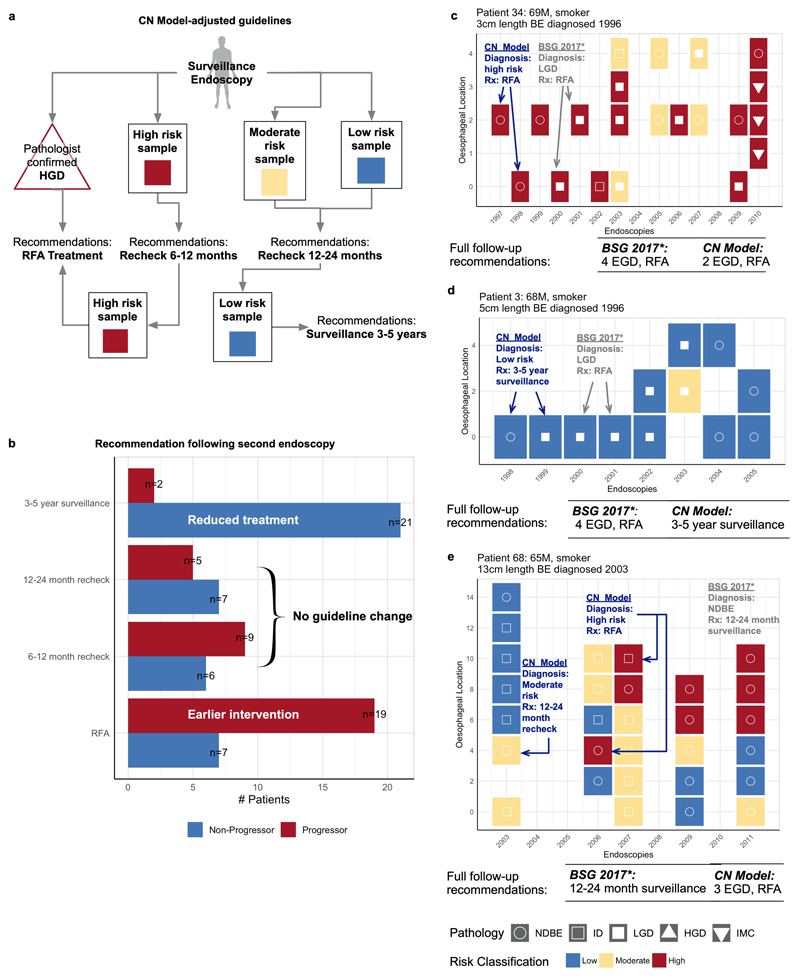
Recent studies show that aneuploidy and driver gene mutations precede cancer diagnosis by many years1-4. We assess whether these genomic signals can be used for early detection and pre-emptive cancer treatment using the neoplastic precursor lesion Barrett's esophagus as an exemplar5. Shallow whole-genome sequencing of 777 biopsies, sampled from 88 patients in Barrett's esophagus surveillance over a period of up to 15 years, shows that genomic signals can distinguish progressive from stable disease even 10 years before histopathological transformation. These findings are validated on two independent cohorts of 76 and 248 patients. These methods are low-cost and applicable to standard clinical biopsy samples. Compared with current management guidelines based on histopathology and clinical presentation, genomic classification enables earlier treatment for high-risk patients as well as reduction of unnecessary treatment and monitoring for patients who are unlikely to develop cancer.
Figures
Comment in
-
A genomic instability-based model for Barrett's oesophagus progression.Nat Rev Clin Oncol. 2020 Nov;17(11):654. doi: 10.1038/s41571-020-00436-2. Nat Rev Clin Oncol. 2020. PMID: 32943767 No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
