

Altered Hemodynamics and End-Organ Damage in Heart Failure: Impact on the Lung and Kidney
- PMID: 32897746
- PMCID: PMC7482031
- DOI: 10.1161/CIRCULATIONAHA.119.045409
Altered Hemodynamics and End-Organ Damage in Heart Failure: Impact on the Lung and Kidney
Abstract
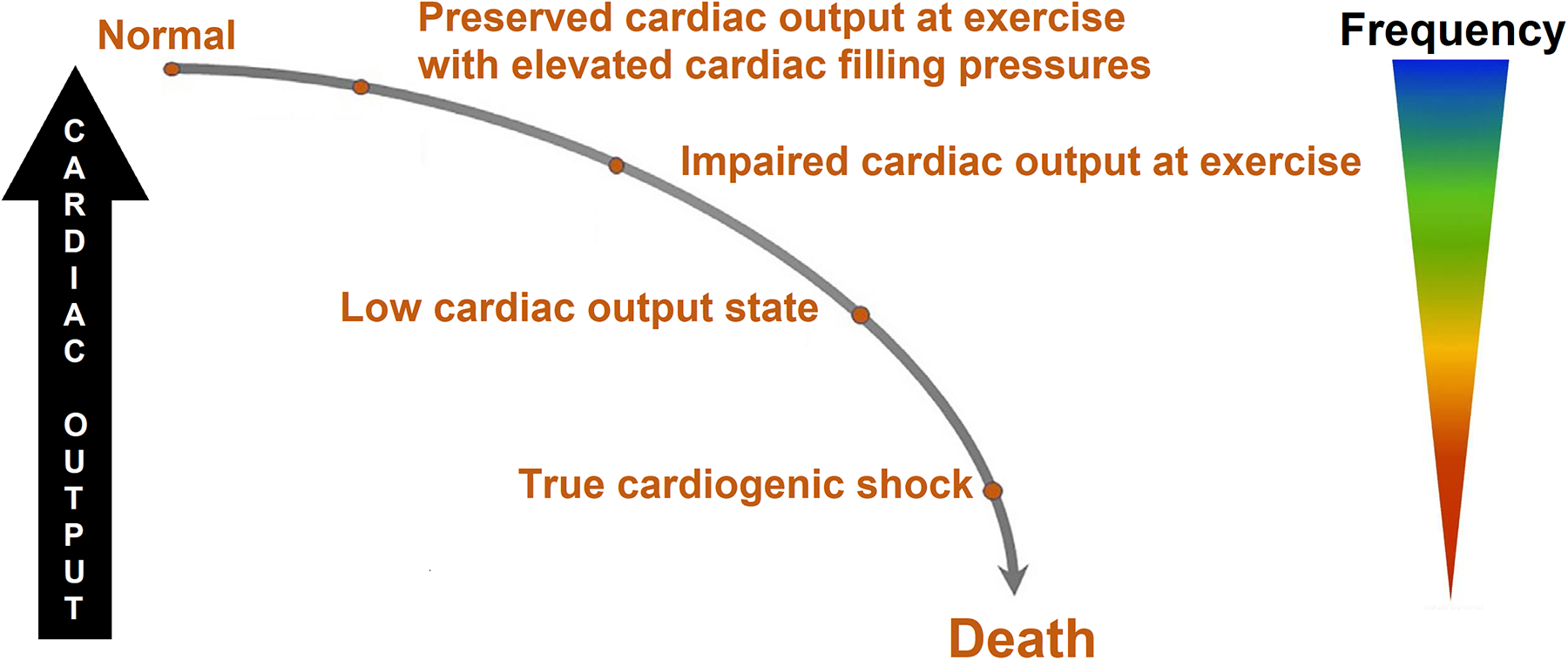
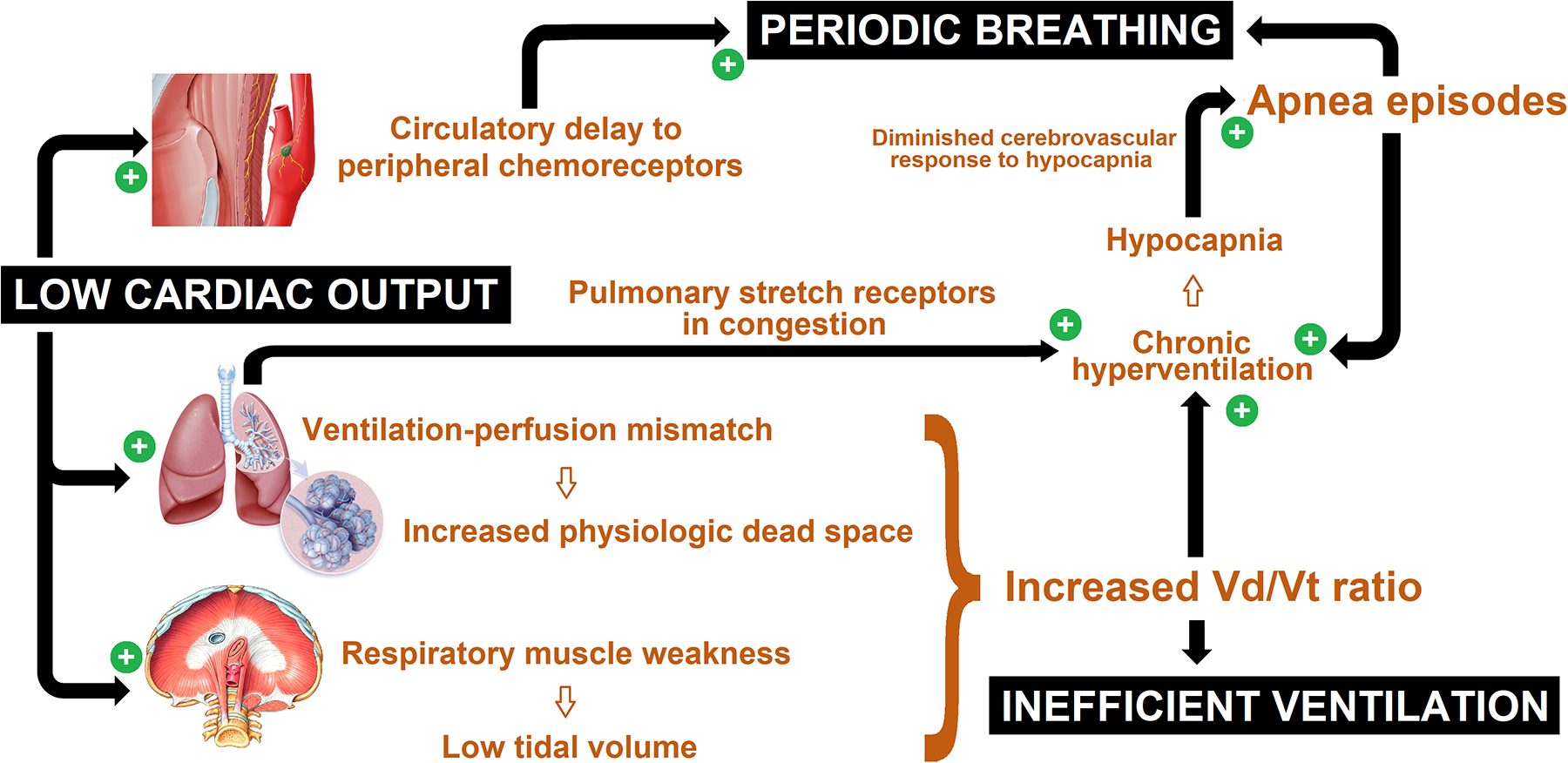
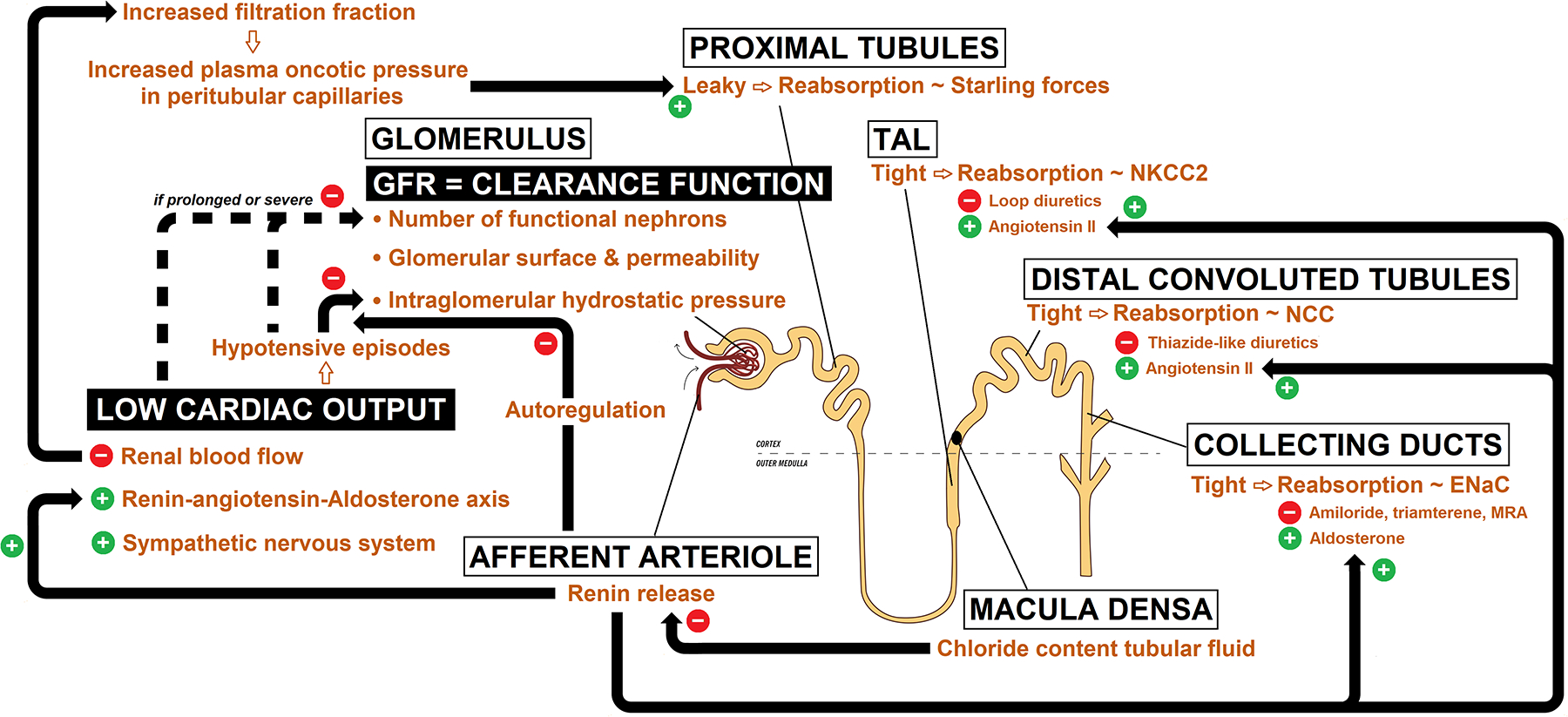
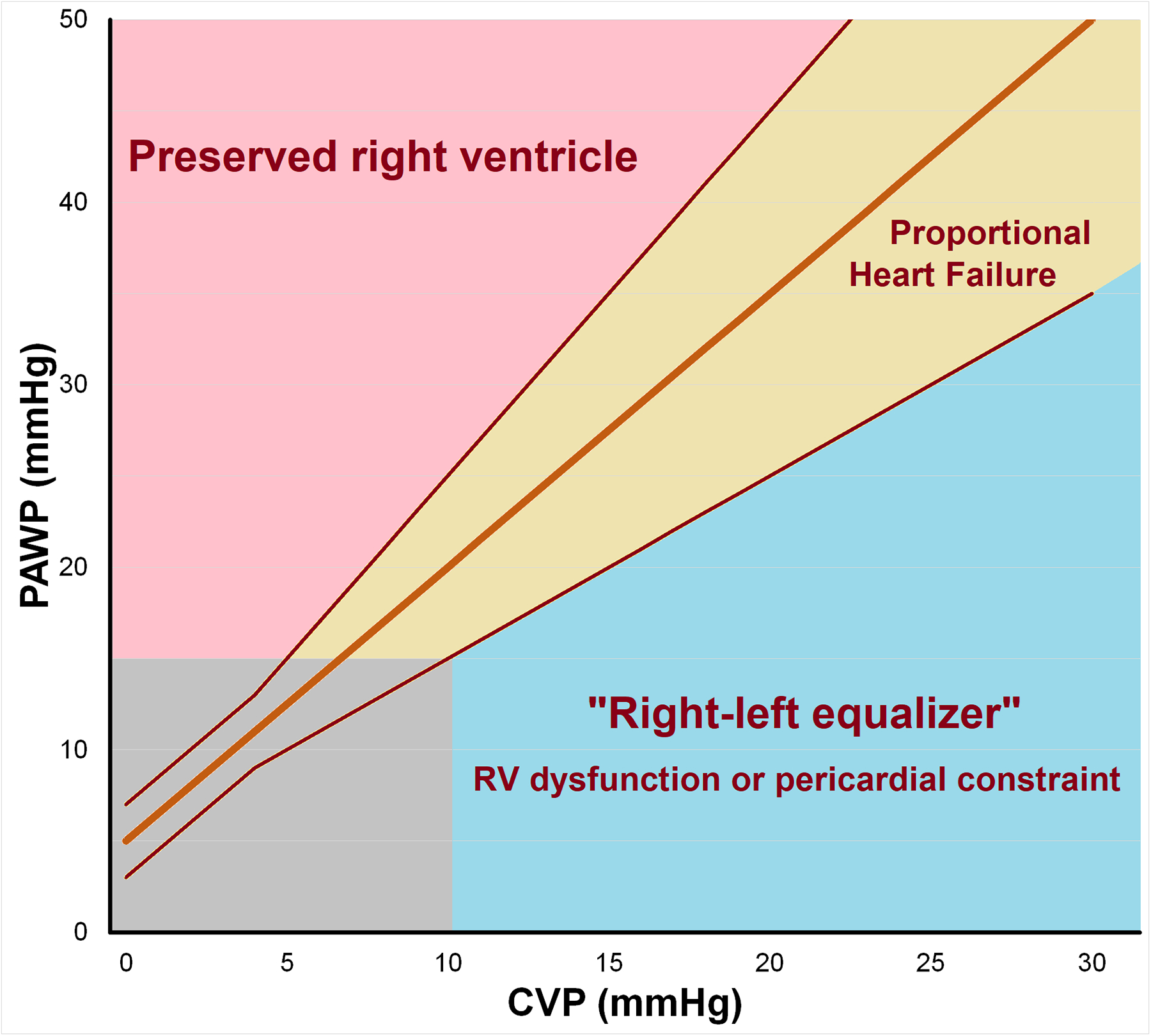
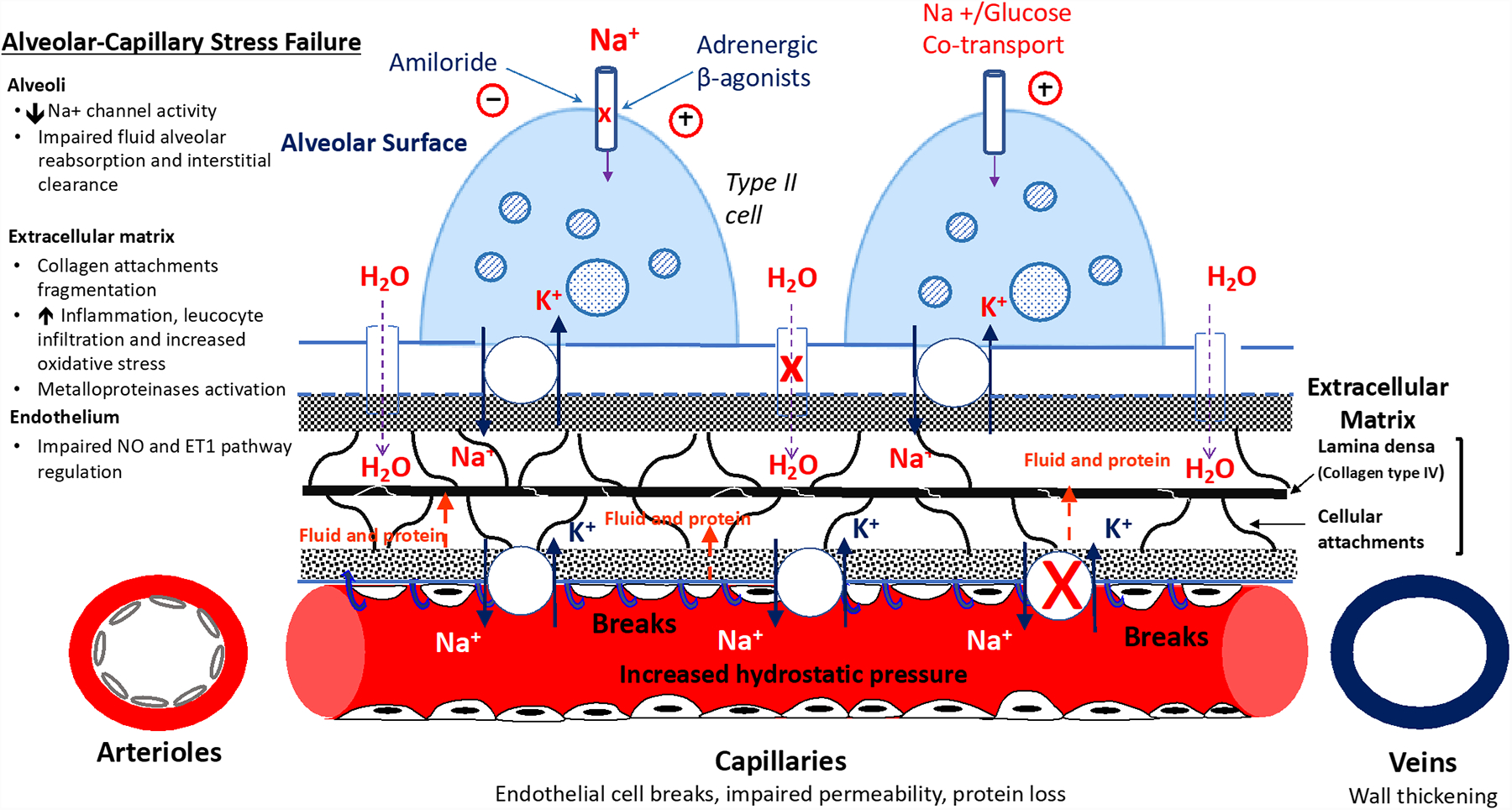
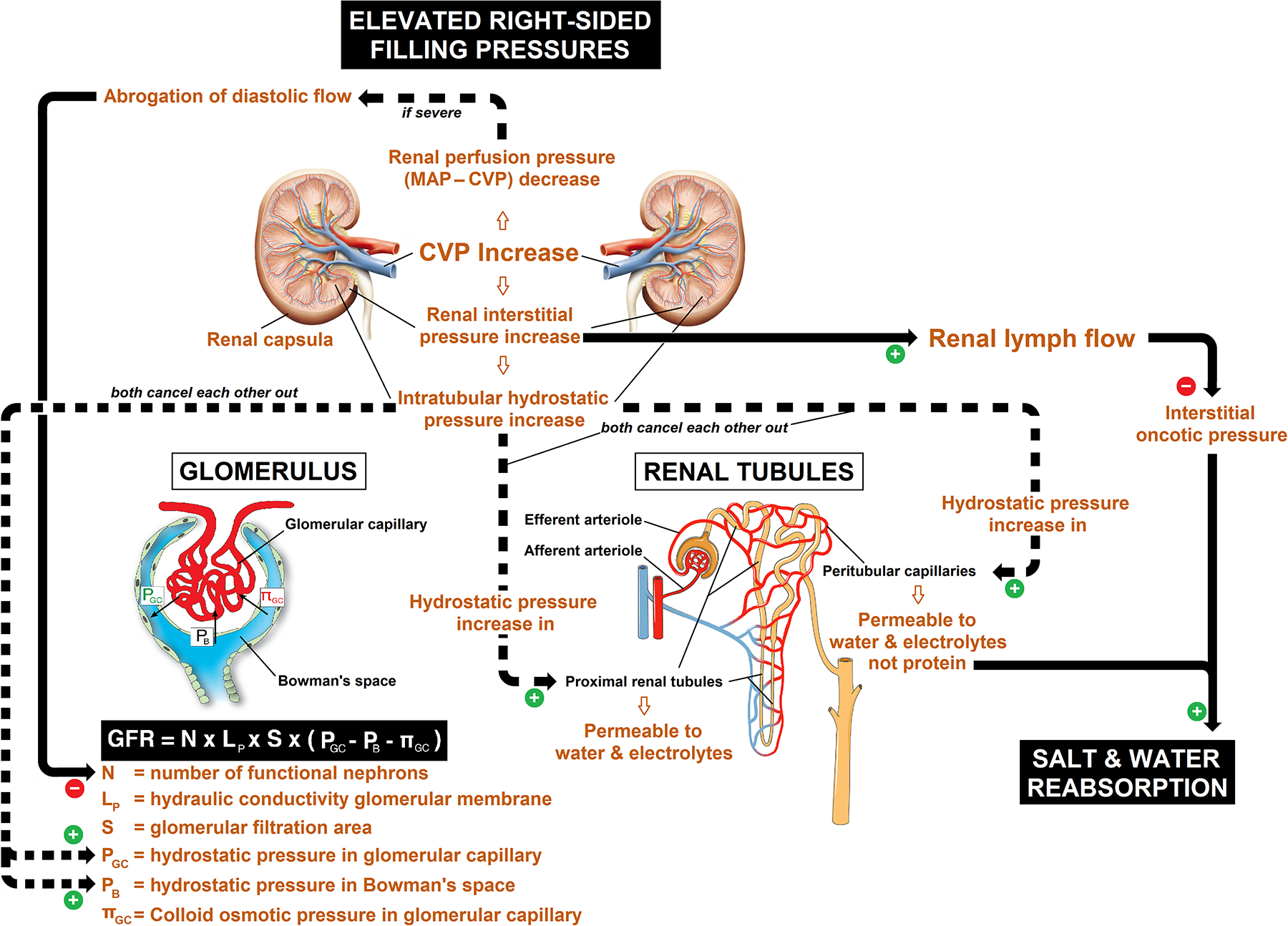
Heart failure is characterized by pathologic hemodynamic derangements, including elevated cardiac filling pressures ("backward" failure), which may or may not coexist with reduced cardiac output ("forward" failure). Even when normal during unstressed conditions such as rest, hemodynamics classically become abnormal during stressors such as exercise in patients with heart failure. This has important upstream and downstream effects on multiple organ systems, particularly with respect to the lungs and kidneys. Hemodynamic abnormalities in heart failure are affected by processes that extend well beyond the cardiac myocyte, including important roles for pericardial constraint, ventricular interaction, and altered venous capacity. Hemodynamic perturbations have widespread effects across multiple heart failure phenotypes, ranging from reduced to preserved ejection fraction, acute to chronic disease, and cardiogenic shock to preserved perfusion states. In the lung, hemodynamic derangements lead to the development of abnormalities in ventilatory control and efficiency, pulmonary congestion, capillary stress failure, and eventually pulmonary vascular disease. In the kidney, hemodynamic perturbations lead to sodium and water retention and worsening renal function. Improved understanding of the mechanisms by which altered hemodynamics in heart failure affect the lungs and kidneys is needed in order to design novel strategies to improve clinical outcomes.
Keywords: heart failure; hemodynamics; kidney; lung.
Conflict of interest statement
Conflict of interest disclosures
None
Figures

References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
