

Brief Preoperative Screening for Frailty and Cognitive Impairment Predicts Delirium after Spine Surgery
- PMID: 32898243
- PMCID: PMC7657972
- DOI: 10.1097/ALN.0000000000003523
Brief Preoperative Screening for Frailty and Cognitive Impairment Predicts Delirium after Spine Surgery
Abstract
Background: Frailty and cognitive impairment are associated with postoperative delirium, but are rarely assessed preoperatively. The study was designed to test the hypothesis that preoperative screening for frailty or cognitive impairment identifies patients at risk for postoperative delirium (primary outcome).
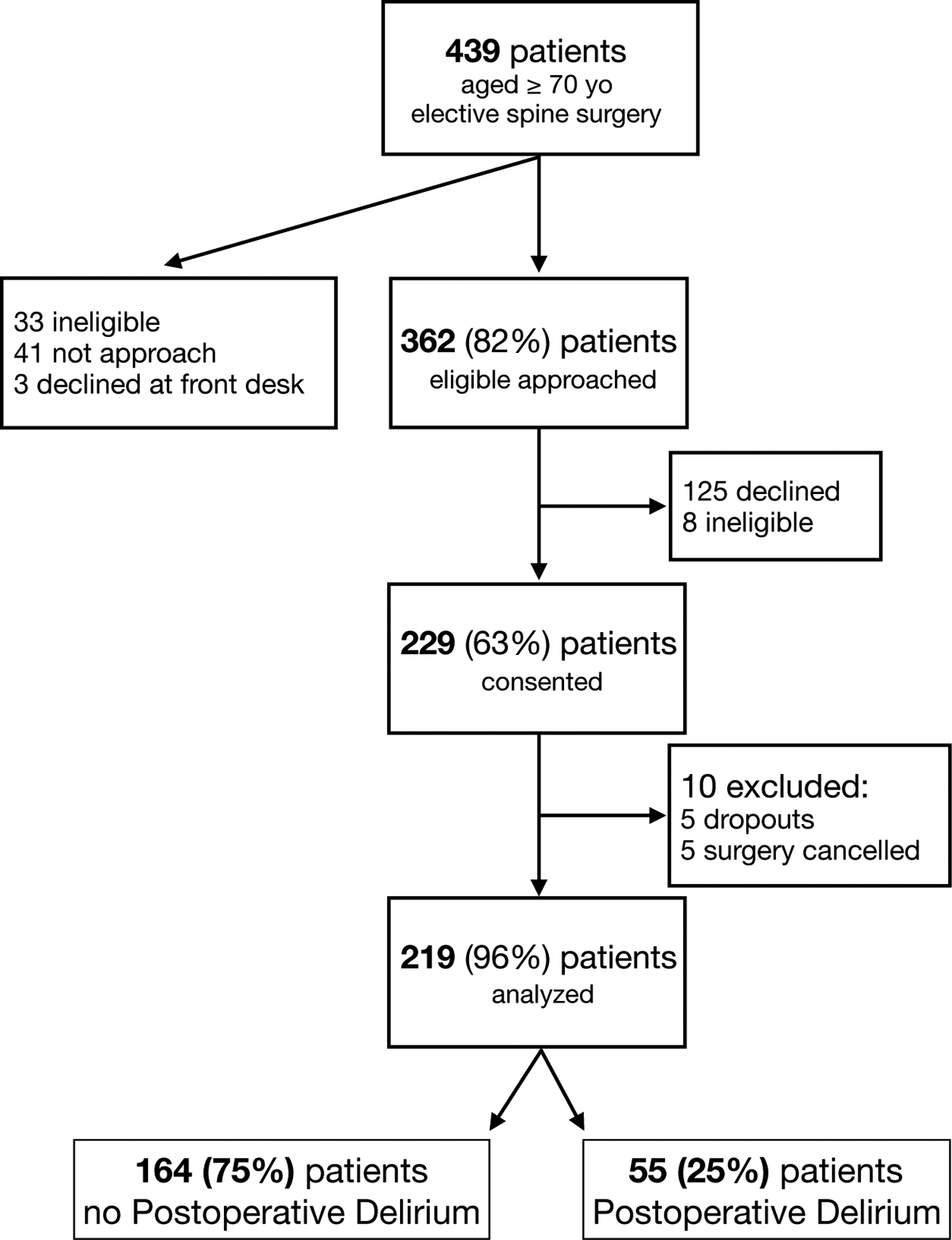
Methods: In this prospective cohort study, the authors administered frailty and cognitive screening instruments to 229 patients greater than or equal to 70 yr old presenting for elective spine surgery. Screening for frailty (five-item FRAIL scale [measuring fatigue, resistance, ambulation, illness, and weight loss]) and cognition (Mini-Cog, Animal Verbal Fluency) were performed at the time of the preoperative evaluation. Demographic data, perioperative variables, and postoperative outcomes were gathered. Delirium was the primary outcome detected by either the Confusion Assessment Method, assessed daily from postoperative day 1 to 3 or until discharge, if patient was discharged sooner, or comprehensive chart review. Secondary outcomes were all other-cause complications, discharge not to home, and hospital length of stay.
Results: The cohort was 75 [73 to 79 yr] years of age, 124 of 219 (57%) were male. Many scored positive for prefrailty (117 of 218; 54%), frailty (53 of 218; 24%), and cognitive impairment (50 to 82 of 219; 23 to 37%). Fifty-five patients (25%) developed delirium postoperatively. On multivariable analysis, frailty (scores 3 to 5 [odds ratio, 6.6; 95% CI, 1.96 to 21.9; P = 0.002]) versus robust (score 0) on the FRAIL scale, lower animal fluency scores (odds ratio, 1.08; 95% CI, 1.01 to 1.51; P = 0.036) for each point decrease in the number of animals named, and more invasive surgical procedures (odds ratio, 2.69; 95% CI, 1.31 to 5.50; P = 0.007) versus less invasive procedures were associated with postoperative delirium.
Conclusions: Screening for frailty and cognitive impairment preoperatively using the FRAIL scale and the Animal Verbal Fluency test in older elective spine surgery patients identifies those at high risk for the development of postoperative delirium.
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved.
Conflict of interest statement
Conflicts of Interest:
MJS: None
RHG: None
BR: None
JDK: None
TRS: None
YL: None
MWG: None
JHC: None
FG: None
DJC: Director of the American Board of Anesthesiology, Member ABMS Committee on Continuous Certification, ACGME – RRC ex-officio member, Executive Editor Anesthesiology, ASA committee member; Grant funding: NIA, NIGMS.
Figures
Comment in
-
Preoperative Frailty and Cognitive Dysfunction Assessment.Anesthesiology. 2020 Dec 1;133(6):1164-1166. doi: 10.1097/ALN.0000000000003579. Anesthesiology. 2020. PMID: 33395463 No abstract available.
References
-
- Inouye SK: Delirium in older persons. N Engl J Med 2006; 354: 1157–65 - PubMed
-
- Chow WB, Rosenthal RA, Merkow RP, Ko CY, Esnaola NF, American College of Surgeons National Surgical Quality Improvement P, American Geriatrics S: Optimal preoperative assessment of the geriatric surgical patient: a best practices guideline from the American College of Surgeons National Surgical Quality Improvement Program and the American Geriatrics Society. J Am Coll Surg 2012; 215: 453–66 - PubMed
-
- Aldecoa C, Bettelli G, Bilotta F, Sanders RD, Audisio R, Borozdina A, Cherubini A, Jones C, Kehlet H, MacLullich A, Radtke F, Riese F, Slooter AJ, Veyckemans F, Kramer S, Neuner B, Weiss B, Spies CD: European Society of Anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur J Anaesthesiol 2017; 34: 192–214 - PubMed
-
- Woo J, Yu R, Wong M, Yeung F, Wong M, Lum C: Frailty Screening in the Community Using the FRAIL Scale. J Am Med Dir Assoc 2015; 16: 412–9 - PubMed
