

Review
doi: 10.1097/ALN.0000000000003547.
Genomic Screening for Malignant Hyperthermia Susceptibility
- PMID: 32898259
- PMCID: PMC7658016
- DOI: 10.1097/ALN.0000000000003547
Item in Clipboard
Review
Genomic Screening for Malignant Hyperthermia Susceptibility
Anesthesiology.
.
Abstract
It is timely to consider the utility and practicability of screening for malignant hyperthermia susceptibility using genomic testing. Here the authors pose a simple, but bold question: what would it take to end deaths from malignant hyperthermia? The authors review recent advances and propose a scientific and clinical pathway toward this audacious goal to provoke discussion in the field.
Copyright © 2020, the American Society of Anesthesiologists, Inc. All Rights Reserved.
Figures
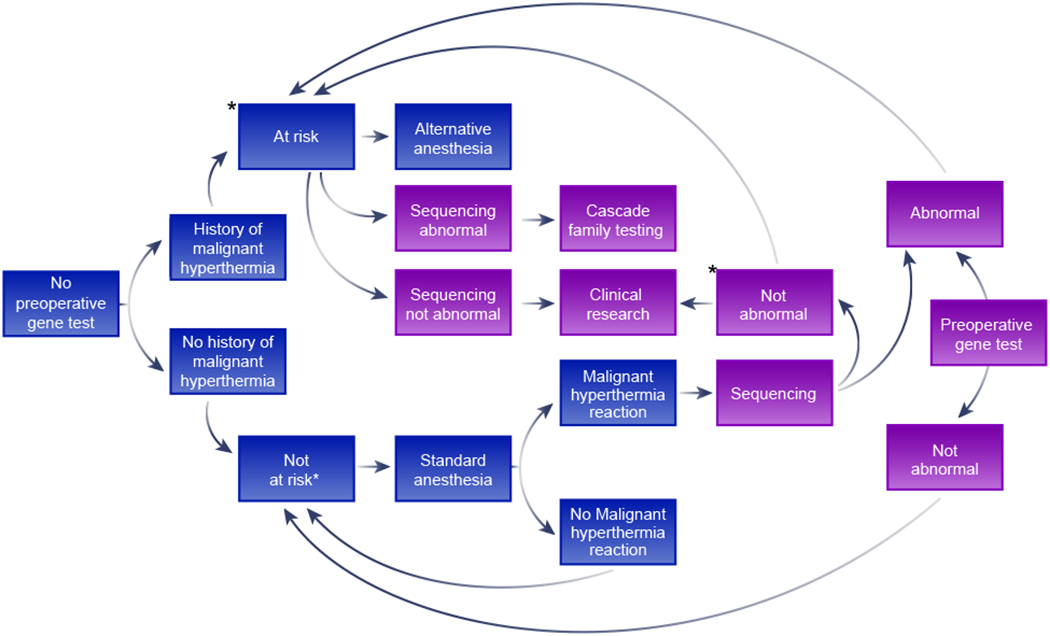
A model for the future management of malignant hyperthermia susceptibility risk through genomic screening. The blue boxes represent the current, phenotypic ascertainment approach to malignant hyperthermia susceptibility, where neither contracture tests nor DNA testing is practical and the purple boxes represent the proposed future approach, supplementing the present approach. ‘Abnormal testing’ means the presence of a variant that is likely to cause malignant hyperthermia susceptibility. ‘Not abnormal testing’ is the converse of that result. Boxes with an asterisk indicate steps that contracture testing should be considered to assess malignant hyperthermia risk. Note that contracture testing may be done prior to DNA testing or reserved for those who show no abnormality on sequencing. The phrase ‘history of malignant hyperthermia’ should be considered as at least a reasonably strong history and ‘malignant hyperthermia reaction’ should be considered as at least reasonably strong evidence of a malignant hyperthermia reaction.
Comment in
-
Definitive diagnosis of malignant hyperthermia susceptibility by genetic testing: A case report.Paediatr Anaesth. 2023 Oct;33(10):868-869. doi: 10.1111/pan.14714. Epub 2023 Jun 26. Paediatr Anaesth. 2023. PMID: 37357724 No abstract available.
References
-
- Rosenberg H, Sambuughin N, Riazi S, Dirksen R: Malignant Hyperthermia Susceptibility, GeneReviews((R)). Edited by Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K, Amemiya A. Seattle (WA), 1993 - PubMed
-
- Glahn KP, Ellis FR, Halsall PJ, Muller CR, Snoeck MM, Urwyler A, Wappler F, European Malignant Hyperthermia G: Recognizing and managing a malignant hyperthermia crisis: guidelines from the European Malignant Hyperthermia Group. Br J Anaesth 2010; 105: 417–20 - PubMed
-
- Larach MG, Dirksen SJ, Belani KG, Brandom BW, Metz KM, Policastro MA, Rosenberg H, Valedon A, Watson CB, Society for Ambulatory A, Malignant Hyperthermia Association of the United S, Ambulatory Surgery F, Society for Academic Emergency M, National Association of Emergency Medical T: Special article: Creation of a guide for the transfer of care of the malignant hyperthermia patient from ambulatory surgery centers to receiving hospital facilities. Anesth Analg 2012; 114: 94–100 - PubMed
-
- Larach MG, Brandom BW, Allen GC, Gronert GA, Lehman EB: Cardiac arrests and deaths associated with malignant hyperthermia in north america from 1987 to 2006: a report from the north american malignant hyperthermia registry of the malignant hyperthermia association of the United States. Anesthesiology 2008; 108: 603–11 - PubMed
-
- Rosero EB, Adesanya AO, Timaran CH, Joshi GP: Trends and outcomes of malignant hyperthermia in the United States, 2000 to 2005. Anesthesiology 2009; 110: 89–94 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
