

Impact of SARS-CoV-2 Pandemic on Colorectal Cancer Screening Delay: Effect on Stage Shift and Increased Mortality
- PMID: 32898707
- PMCID: PMC7474804
- DOI: 10.1016/j.cgh.2020.09.008
Impact of SARS-CoV-2 Pandemic on Colorectal Cancer Screening Delay: Effect on Stage Shift and Increased Mortality
Abstract
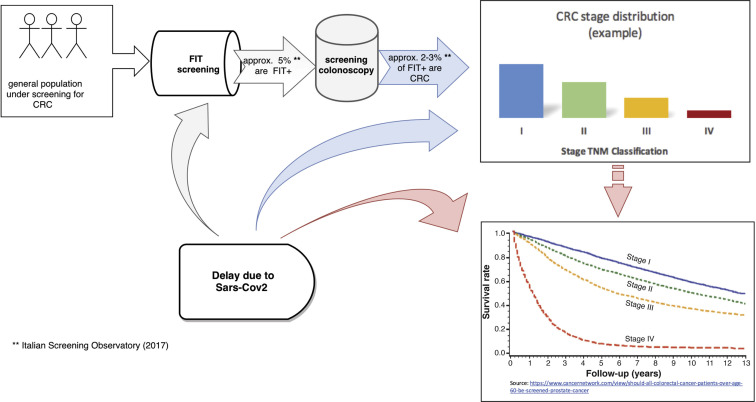
Background & aims: The SARS-CoV-2 pandemic had a sudden, dramatic impact on healthcare. In Italy, since the beginning of the pandemic, colorectal cancer (CRC) screening programs have been forcefully suspended. We aimed to evaluate whether screening procedure delays can affect the outcomes of CRC screening.
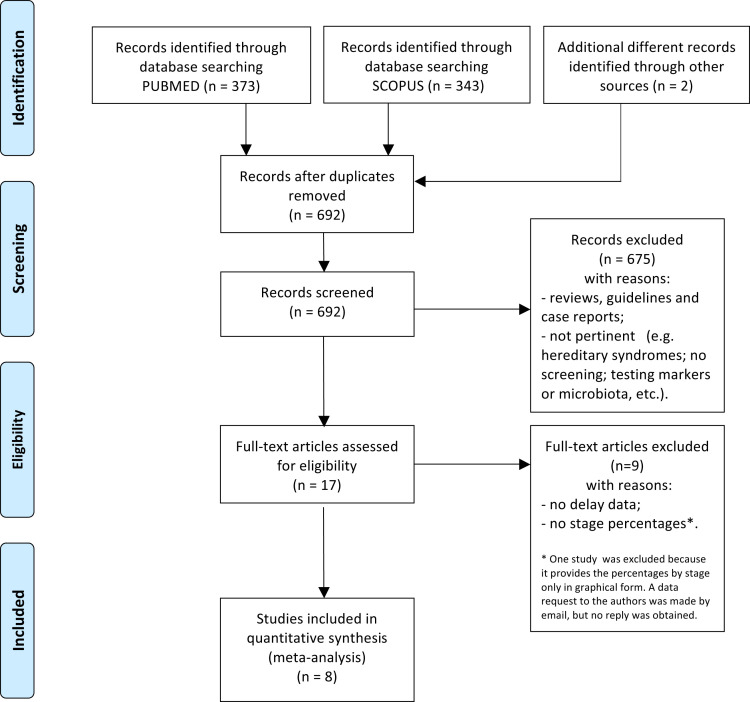
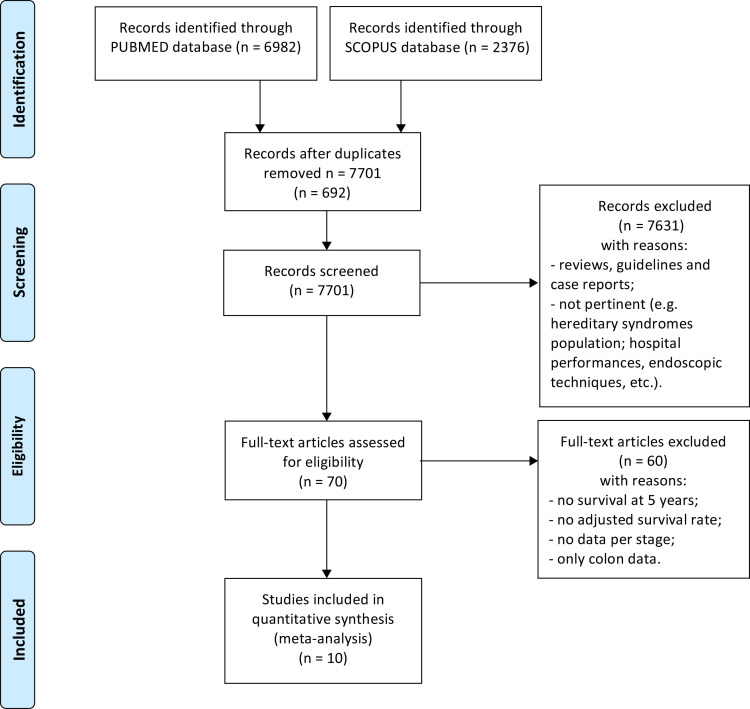
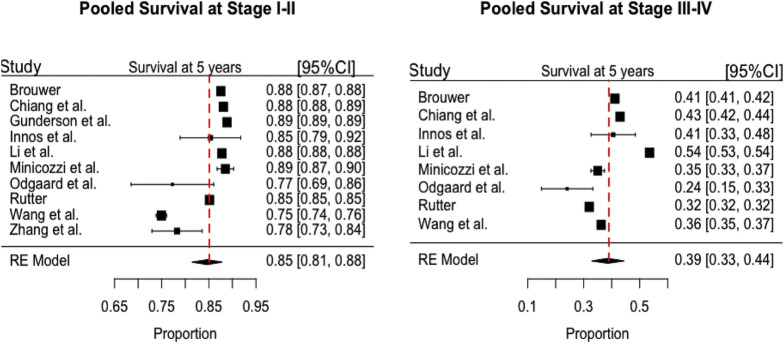
Methods: We built a procedural model considering delays in the time to colonoscopy and estimating the effect on mortality due to up-stage migration of patients. The number of expected CRC cases was computed by using the data of the Italian screened population. Estimates of the effects of delay to colonoscopy on CRC stage, and of stage on mortality were assessed by a meta-analytic approach.
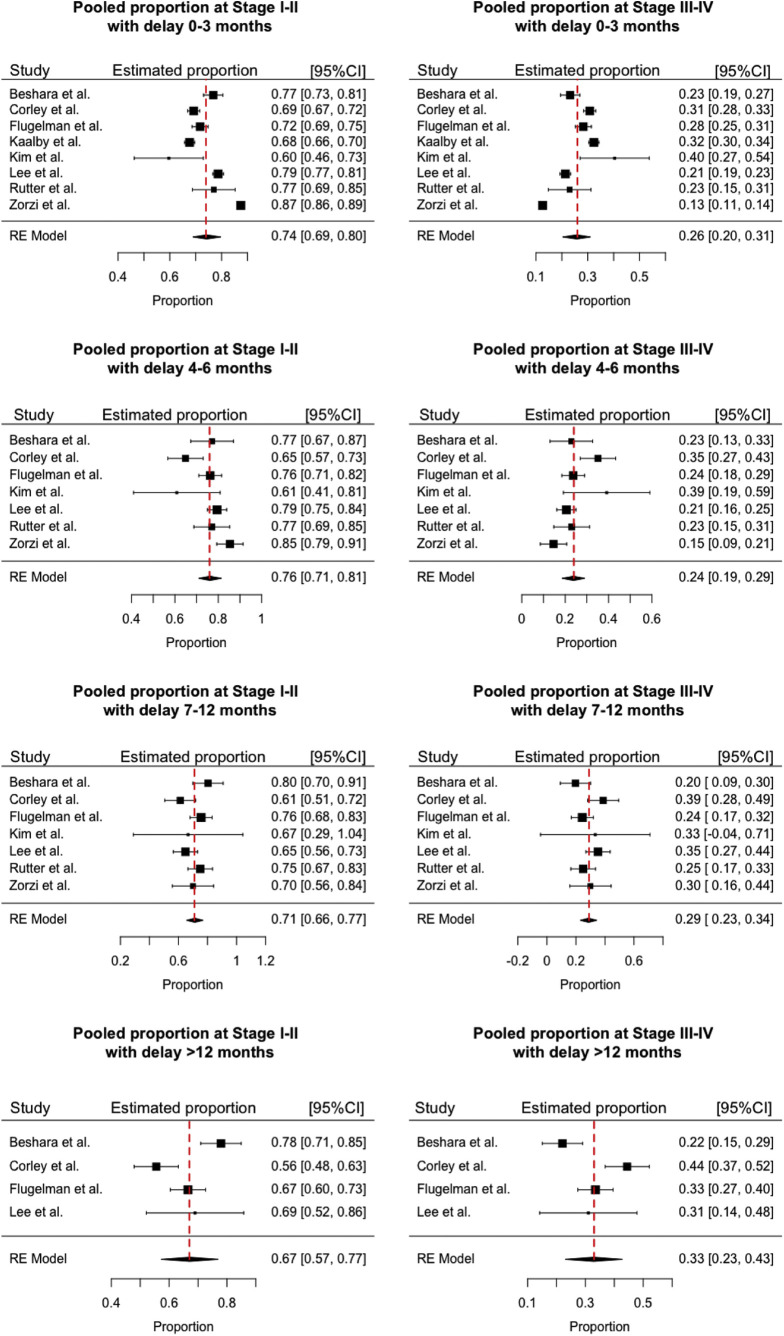
Results: With a delay of 0-3 months, 74% of CRC is expected to be stage I-II, while with a delay of 4-6 months there would be a 2%-increase for stage I-II and a concomitant decrease for stage III-IV (P = .068). Compared to baseline (0-3 months), moderate (7-12 months) and long (> 12 months) delays would lead to a significant increase in advanced CRC (from 26% to 29% and 33%, respectively; P = .008 and P < .001, respectively). We estimated a significant increase in the total number of deaths (+12.0%) when moving from a 0-3-months to a >12-month delay (P = .005), and a significant change in mortality distribution by stage when comparing the baseline with the >12-months (P < .001).
Conclusions: Screening delays beyond 4-6 months would significantly increase advanced CRC cases, and also mortality if lasting beyond 12 months. Our data highlight the need to reorganize efforts against high-impact diseases such as CRC, considering possible future waves of SARS-CoV-2 or other pandemics.
Keywords: Colon Cancer; Colonoscopy; Colorectal Cancer Screening; Fecal Immunochemical Test; SARS-CoV-2.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
COVID-19 and digestive health: Implications for prevention, care and the use of COVID-19 vaccines in vulnerable patients.United European Gastroenterol J. 2021 Nov;9(9):1091-1095. doi: 10.1002/ueg2.12173. Epub 2021 Oct 30. United European Gastroenterol J. 2021. PMID: 34716760 Free PMC article. No abstract available.
References
-
- Hick J.L., Biddinger P.D. Novel coronavirus and old lessons: preparing the health system for the pandemic. N Engl J Med. 2020;382:e55. - PubMed
-
- Bray F., Ferlay J., Soerjomataram I. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. - PubMed
-
- Senore C., Basu P., Anttila A. Performance of colorectal cancer screening in the European Union Member States: data from the second European screening report. Gut. 2019;68:1232–1244. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
