

Subaxial Vertebral Artery Rotational Occlusion Syndrome: An Overview of Clinical Aspects, Diagnostic Work-Up, and Surgical Management
- PMID: 32898967
- PMCID: PMC8217850
- DOI: 10.31616/asj.2020.0275
Subaxial Vertebral Artery Rotational Occlusion Syndrome: An Overview of Clinical Aspects, Diagnostic Work-Up, and Surgical Management
Abstract
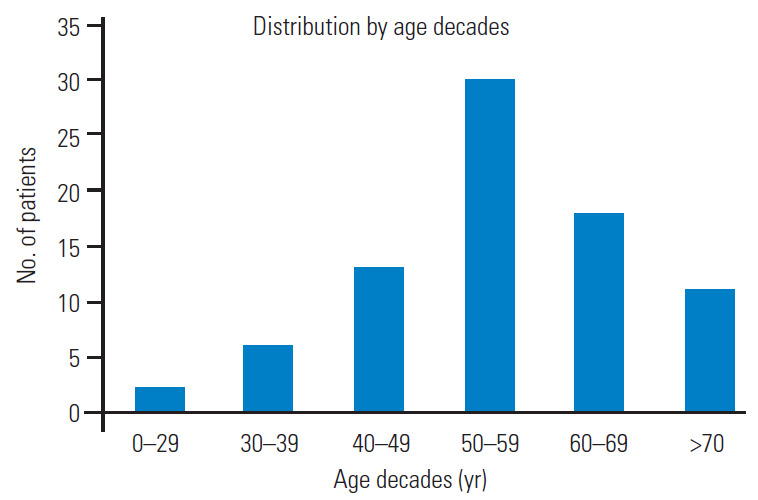
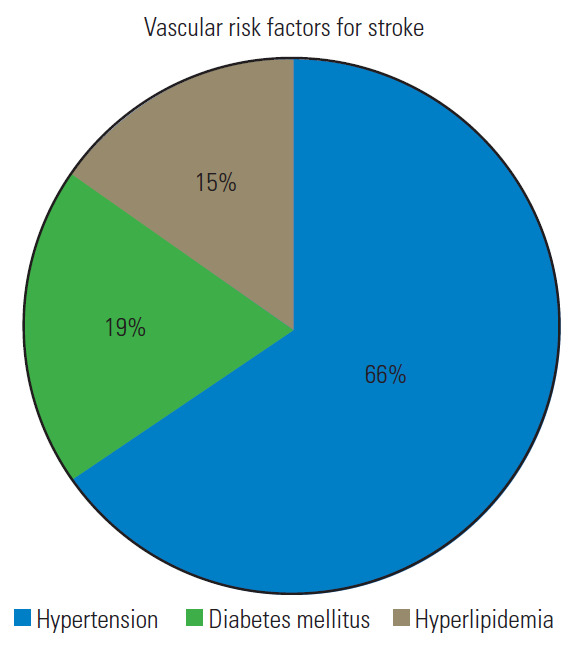
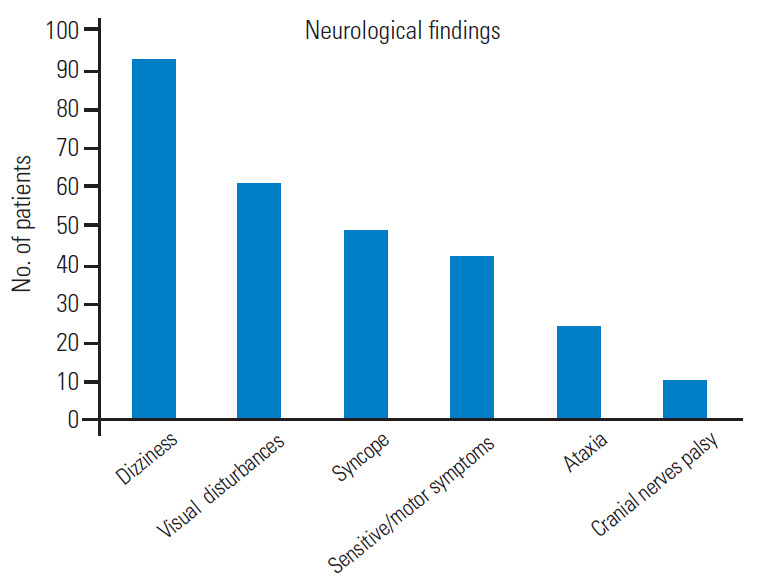
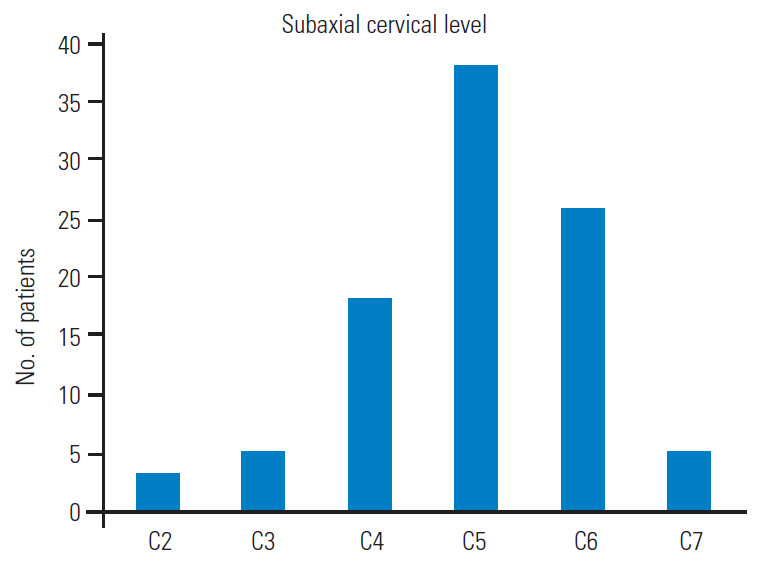
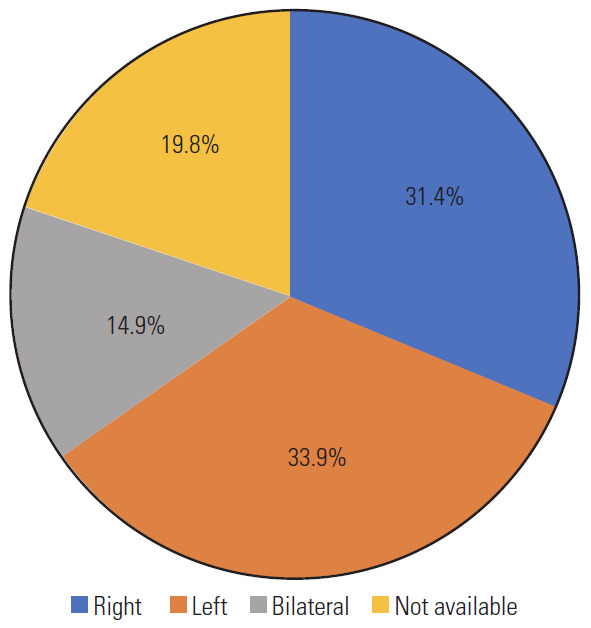
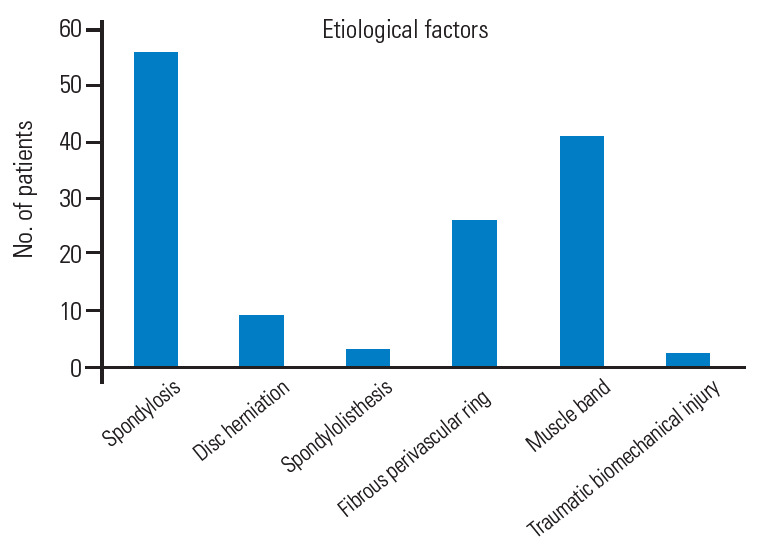
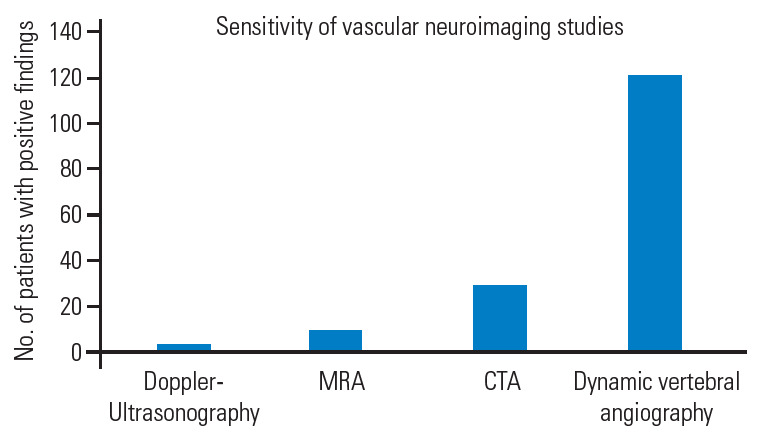
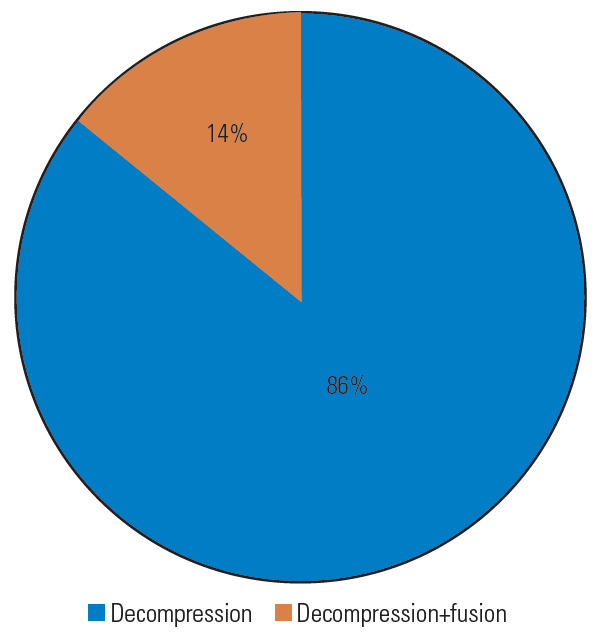
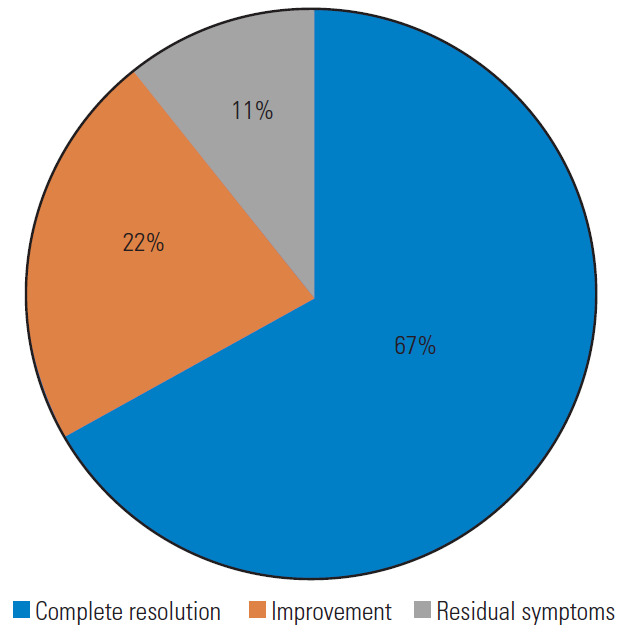
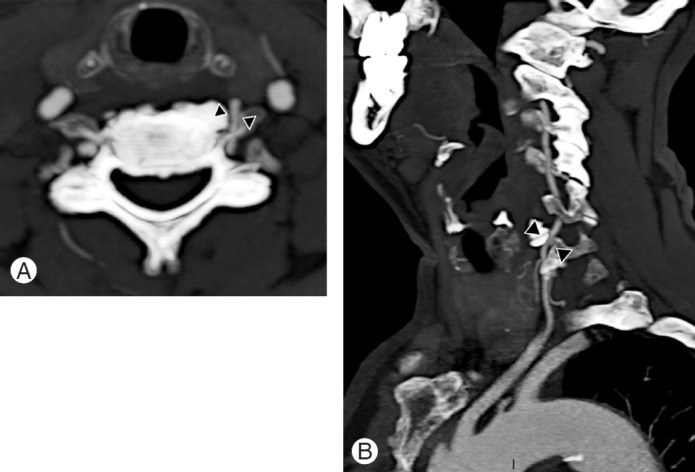
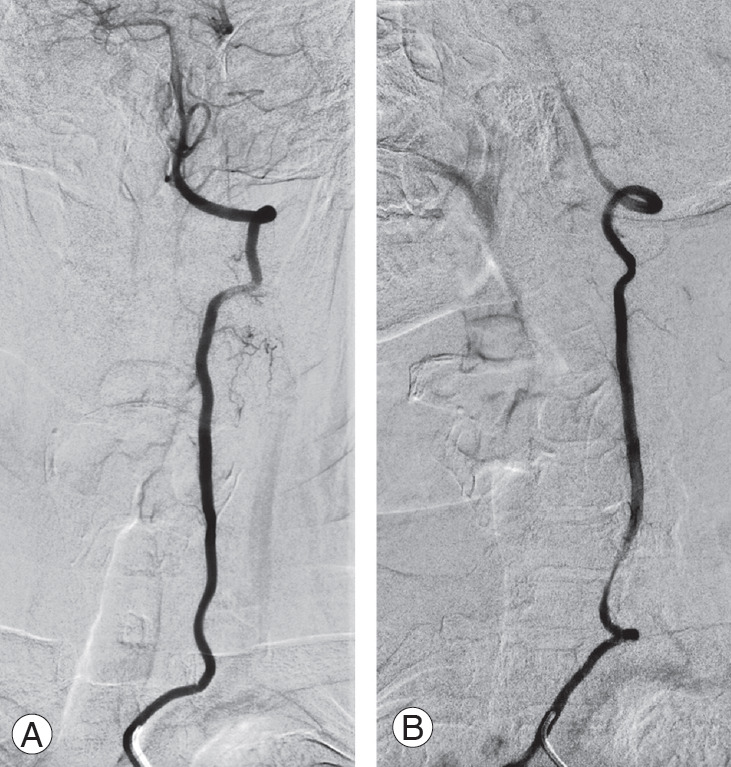
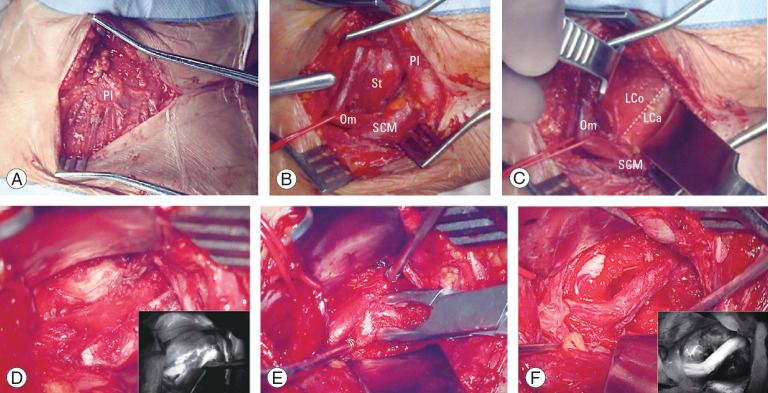
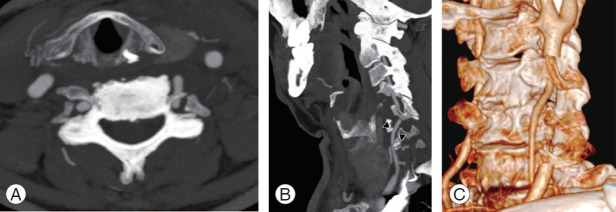
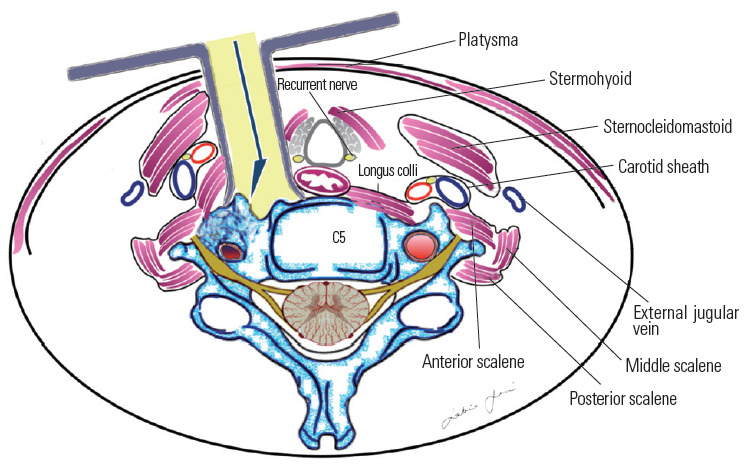
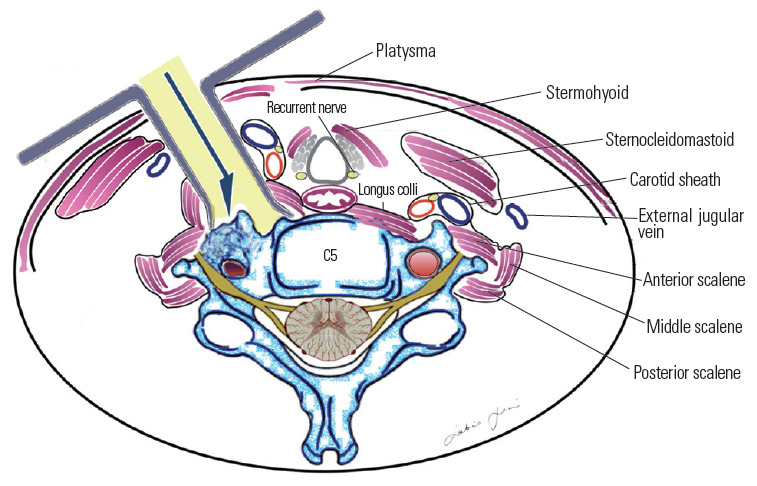
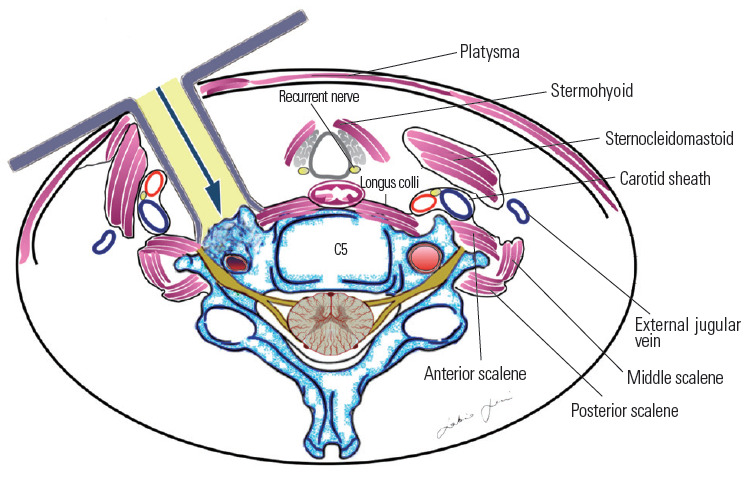
Extrinsic compression of the subaxial vertebral artery (VA) may cause rotational occlusion syndrome (ROS) and contribute to vertebrobasilar insufficiency potentially leading to symptoms and in severe cases, to posterior circulation strokes. The present literature review aimed to report the main clinical findings, diagnostic work-up, and surgical management of the subaxial VA-ROS, the diagnosis of which can be difficult and is often underestimated. An illustrative case is also presented. A thorough literature search was conducted to retrieve manuscripts that have discussed the etiology, diagnosis, and treatment of ROS. Total 41 articles were selected based on the best match and relevance and mainly involved case reports and small cases series. The male/female ratio and average age were 2.6 and 55.6±11 years, respectively. Dizziness, visual disturbances, and syncope were the most frequent symptoms in order of frequency, while C5 and C6 were the most affected levels. Osteophytes were the cause in >46.2% of cases. Dynamic VA catheter-based angiography was the gold standard for diagnosis along with computed tomography angiography. Except in older patients and those with prohibitive comorbidities, anterior decompressive surgery was always performed, mostly with complete recovery, and zero morbidity and mortality. A careful neurological evaluation and dynamic angiographic studies are crucial for the diagnosis of subaxial VA-ROS. Anterior decompression of the VA is the cure of this syndrome in almost all cases.
Keywords: Cerebral angiography; Posterior circulation; Spondylosis; Stroke; Vertebral artery; Vertebrobasilar insufficiency.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Savitz SI, Caplan LR. Vertebrobasilar disease. N Engl J Med. 2005;352:2618–26. - PubMed
-
- Ujifuku K, Hayashi K, Tsunoda K, et al. Positional vertebral artery compression and vertebrobasilar insufficiency due to a herniated cervical disc. J Neurosurg Spine. 2009;11:326–9. - PubMed
-
- Bulsara KR, Velez DA, Villavicencio A. Rotational vertebral artery insufficiency resulting from cervical spondylosis: case report and review of the literature. Surg Neurol. 2006;65:625–7. - PubMed
-
- Sarkar J, Wolfe SQ, Ching BH, Kellicut DC. Bow hunter’s syndrome causing vertebrobasilar insufficiency in a young man with neck muscle hypertrophy. Ann Vasc Surg. 2014;28:1032. - PubMed
-
- Lee V, Riles TS, Stableford J, Berguer R. Two case presentations and surgical management of bow hunter’s syndrome associated with bony abnormalities of the C7 vertebra. J Vasc Surg. 2011;53:1381–5. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
