

Surgical treatment and prognosis of focal brainstem gliomas in children: A 7 year single center experience
- PMID: 32899058
- PMCID: PMC7478697
- DOI: 10.1097/MD.0000000000022029
Surgical treatment and prognosis of focal brainstem gliomas in children: A 7 year single center experience
Abstract
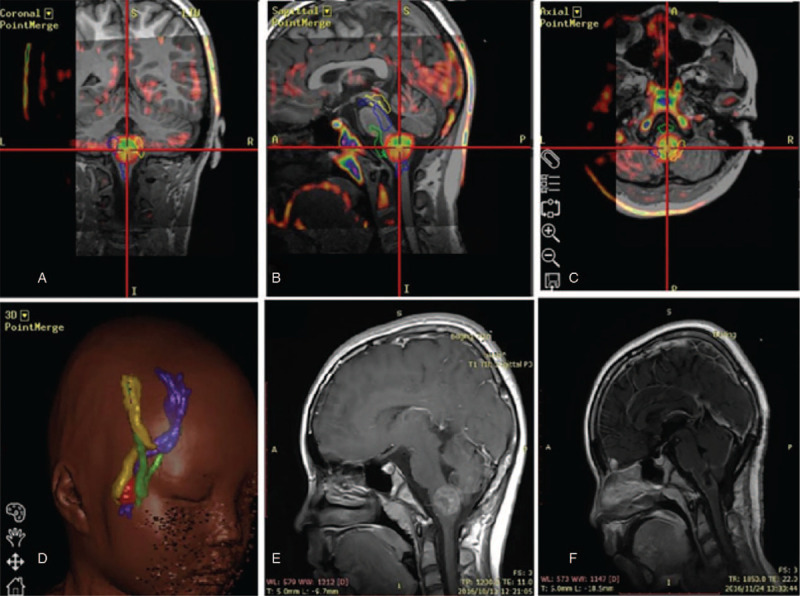
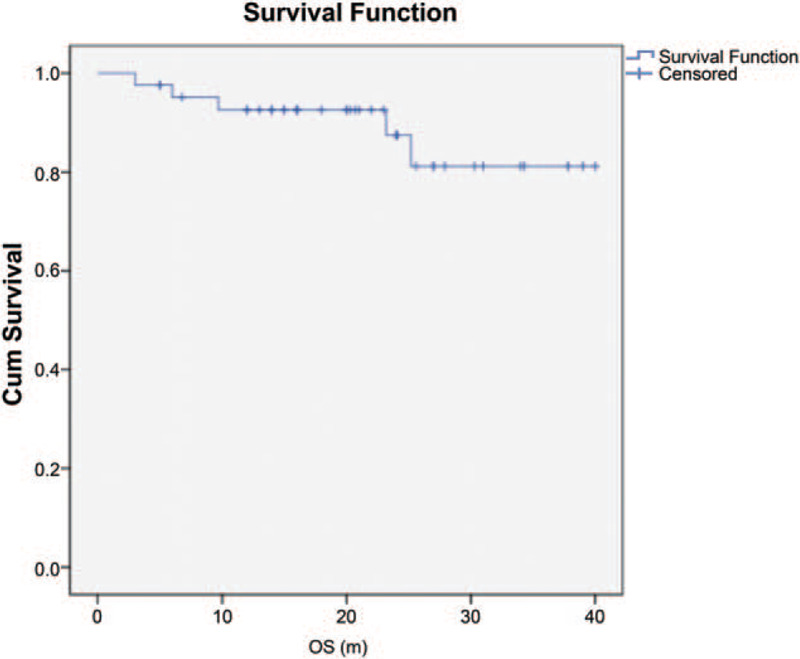
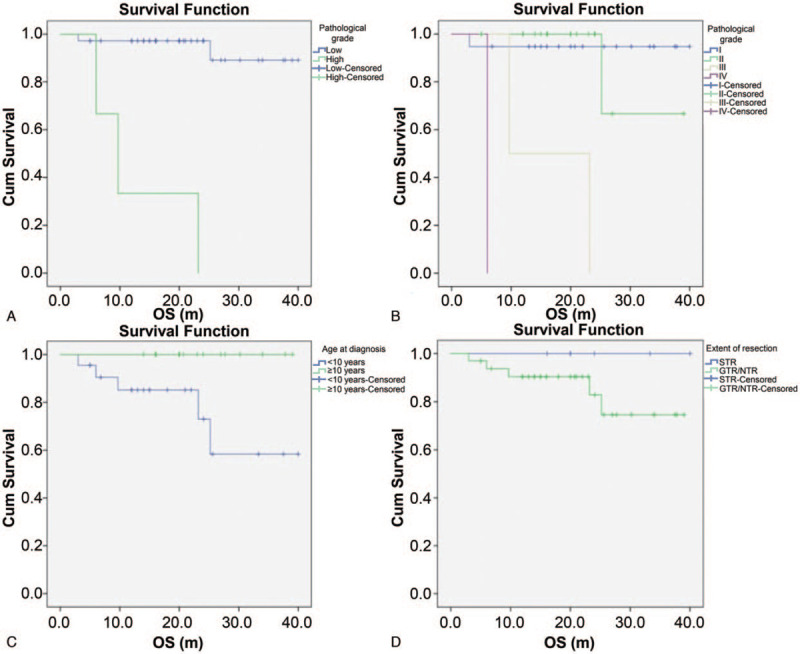
This study aims to describe the role of open surgical treatment for focal brainstem gliomas (FBSGs) with the assistance of multimodal neuronavigation and intraoperative neurophysiological monitoring (IOM) in children to investigate the efficacy of microsurgical treatment in pediatric FBSGs. Also the prognostic factors related to the overall survival (OS) of FBSGs to describe the patient and tumor characteristics relevant to prognosis/outcome were focused on. Clinical data of 63 pediatric patients below 16 years of age with FBSGs admitted to the Neurosurgical Unit of Beijing Tiantan Hospital from January 2012 to December 2018 were retrospectively analyzed. All patients underwent initial surgical treatment, followed by magnetic resonance diffusion tensor imaging (DTI), neuronavigation and IOM. Gross or near total resection (GTR or NTR) was achieved in 57/63 (90.5%) cases, and subtotal resection (STR) was achieved in 6/63 (9.5%) cases. Postoperative adjuvant therapy was received by 27/63 (42.9%) cases. Postoperative pathological examination revealed that 36/63 (57.1%) cases had grade I gliomas, 22/63 (34.9%) had grade II, and 5/63 (8.0%) had grade III-IV gliomas according to the WHO classification. The mean Karnofsky score preoperatively was 60, and at the time of follow-up was 90. Consecutively, 6 cases demonstrated disease progression, and 5 of these were deceased. The OS in all patients was 81.2% at 5 years. Histological grade (P < .001) and age at diagnosis (P = .023) showed significant association with prolonged OS. Multimodal neuronavigation and IOM allow very precise intracranial surgery, contributing to a maximally safe resection that might decrease the postoperative disability and mortality rate. This study also showed that pediatric FBSGs were mostly low-grade tumors with excellent surgical outcomes. Consequently, it is suggested that microsurgery can be used to treat FBSGs in children in order to provide better prognosis and survival outcomes.
Conflict of interest statement
All authors declare that they have no any conflict of interests.
Figures
References
-
- Fisher PG, Breiter SN, Carson BS, et al. A clinicopathologic reappraisal of brain stem tumor classification. Identification of pilocystic astrocytoma and fibrillary astrocytoma as distinct entities. Cancer 2000;89:1569–76.. - PubMed
-
- Barkovich AJ, Krischer J, Kun LE, et al. Brain stem gliomas: a classification system based on magnetic resonance imaging. Pediatr Neurosurg 1990;16:73–83.. - PubMed
-
- Sun B, Wang CC, Wang J. MRI characteristics of midbrain tumours. Neuroradiology 1999;41:158–62.. - PubMed
-
- Moghrabi A, Kerby T, Tien RD, et al. Prognostic value of contrast-enhanced magnetic resonance imaging in brainstem gliomas. Pediatr Neurosurg 1995;23:293–8.. - PubMed
-
- Albright AL, Packer RJ, Zimmerman R, et al. Magnetic resonance scans should replace biopsies for the diagnosis of diffuse brain stem gliomas: a report from the Children's Cancer Group. Neurosurgery 1993;33:1026–9.. discussion 1029-1030. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
