

Pathways of Gastric Carcinogenesis, Helicobacter pylori Virulence and Interactions with Antioxidant Systems, Vitamin C and Phytochemicals
- PMID: 32899442
- PMCID: PMC7503565
- DOI: 10.3390/ijms21176451
Pathways of Gastric Carcinogenesis, Helicobacter pylori Virulence and Interactions with Antioxidant Systems, Vitamin C and Phytochemicals
Abstract
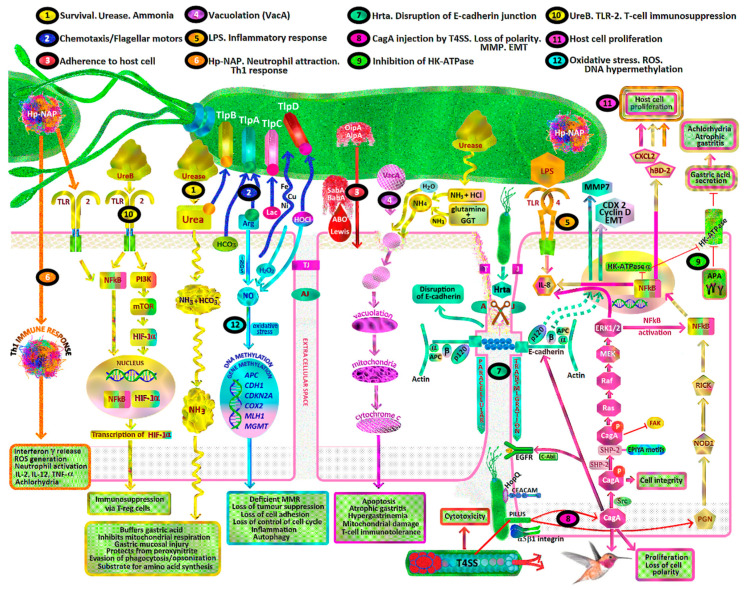
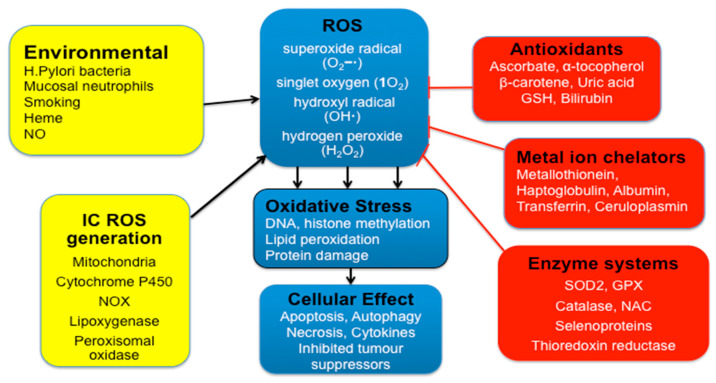
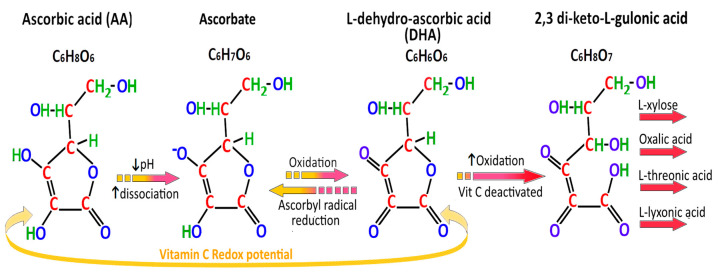
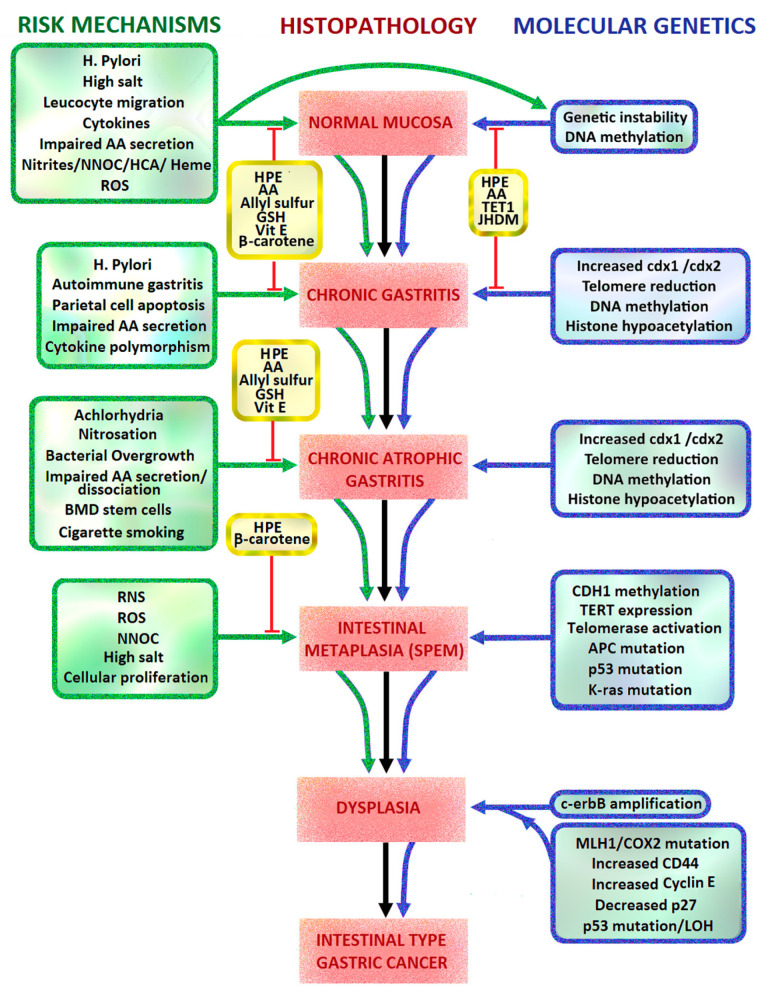
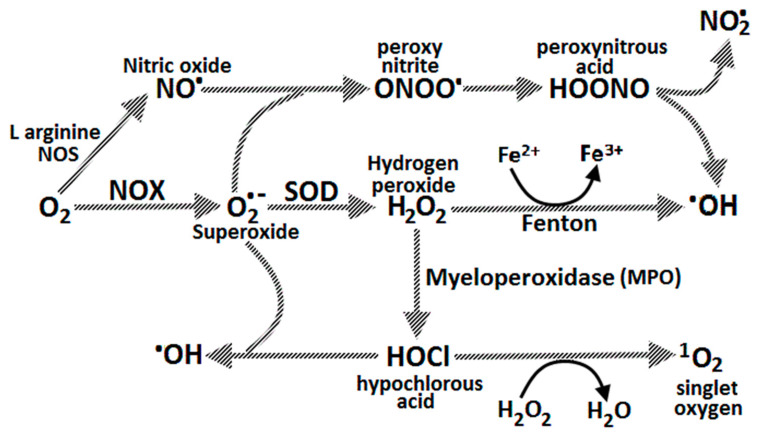
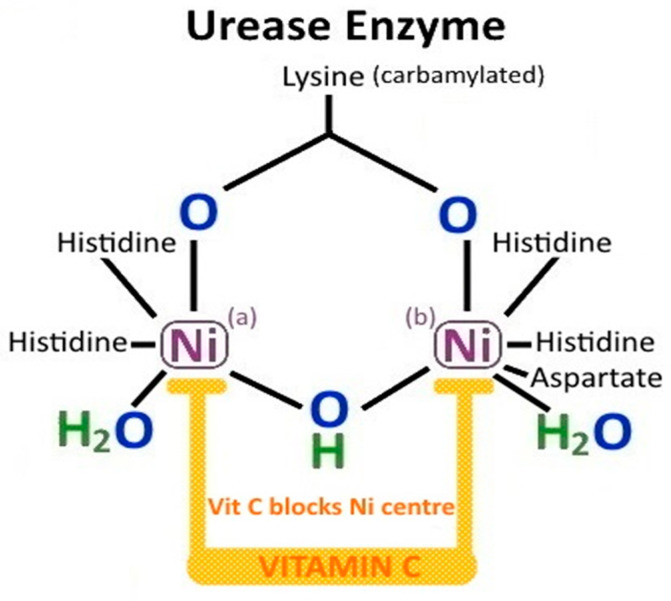
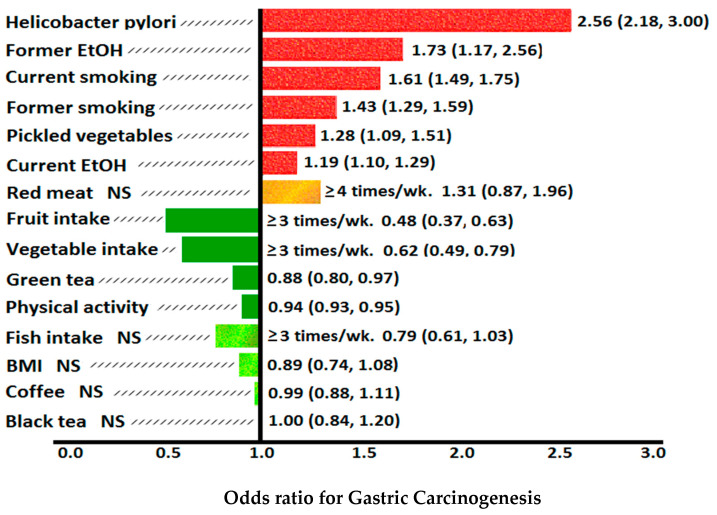
Helicobacter pylori is a class one carcinogen which causes chronic atrophic gastritis, gastric intestinal metaplasia, dysplasia and adenocarcinoma. The mechanisms by which H. pylori interacts with other risk and protective factors, particularly vitamin C in gastric carcinogenesis are complex. Gastric carcinogenesis includes metabolic, environmental, epigenetic, genomic, infective, inflammatory and oncogenic pathways. The molecular classification of gastric cancer subtypes has revolutionized the understanding of gastric carcinogenesis. This includes the tumour microenvironment, germline mutations, and the role of Helicobacter pylori bacteria, Epstein Barr virus and epigenetics in somatic mutations. There is evidence that ascorbic acid, phytochemicals and endogenous antioxidant systems can modify the risk of gastric cancer. Gastric juice ascorbate levels depend on dietary intake of ascorbic acid but can also be decreased by H. pylori infection, H. pylori CagA secretion, tobacco smoking, achlorhydria and chronic atrophic gastritis. Ascorbic acid may be protective against gastric cancer by its antioxidant effect in gastric cytoprotection, regenerating active vitamin E and glutathione, inhibiting endogenous N-nitrosation, reducing toxic effects of ingested nitrosodimethylamines and heterocyclic amines, and preventing H. pylori infection. The effectiveness of such cytoprotection is related to H. pylori strain virulence, particularly CagA expression. The role of vitamin C in epigenetic reprogramming in gastric cancer is still evolving. Other factors in conjunction with vitamin C also play a role in gastric carcinogenesis. Eradication of H. pylori may lead to recovery of vitamin C secretion by gastric epithelium and enable regression of premalignant gastric lesions, thereby interrupting the Correa cascade of gastric carcinogenesis.
Keywords: CagA; Correa pathway; Helicobacter pylori; ascorbic acid; chronic atrophic gastritis; dietary salt; gastric cancer; glutathione; nitrosamines; oxidative stress; phytochemicals; vitamin C.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
