

Triage of Amyotrophic Lateral Sclerosis Patients during the COVID-19 Pandemic: An Application of the D50 Model
- PMID: 32899481
- PMCID: PMC7565659
- DOI: 10.3390/jcm9092873
Triage of Amyotrophic Lateral Sclerosis Patients during the COVID-19 Pandemic: An Application of the D50 Model
Abstract
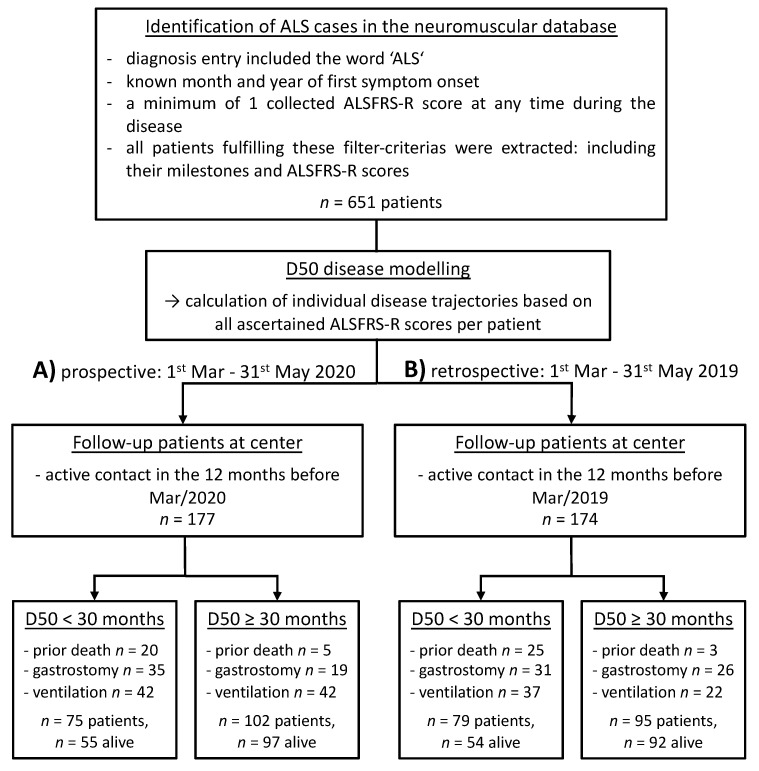
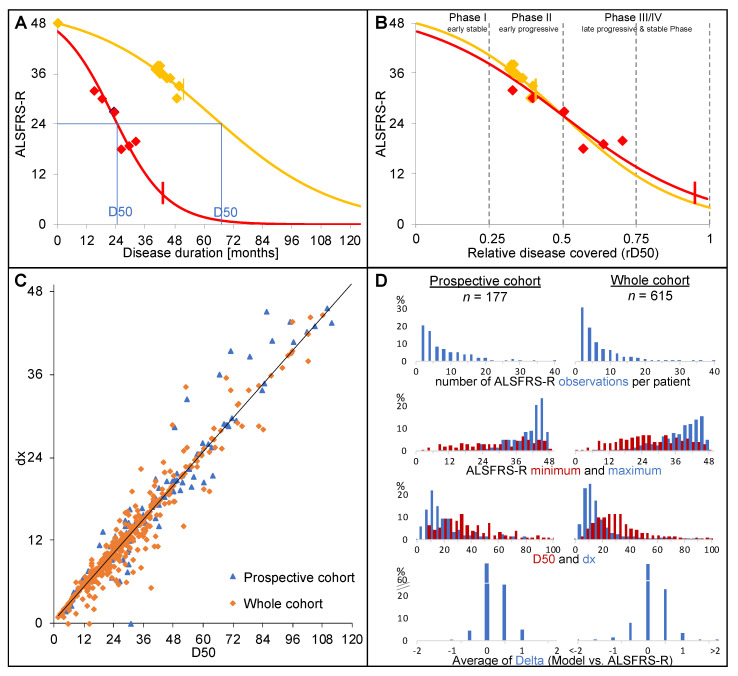
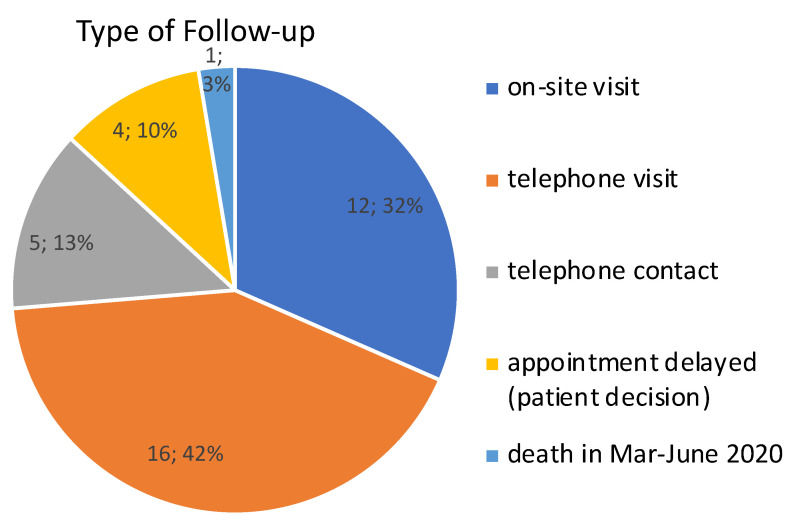
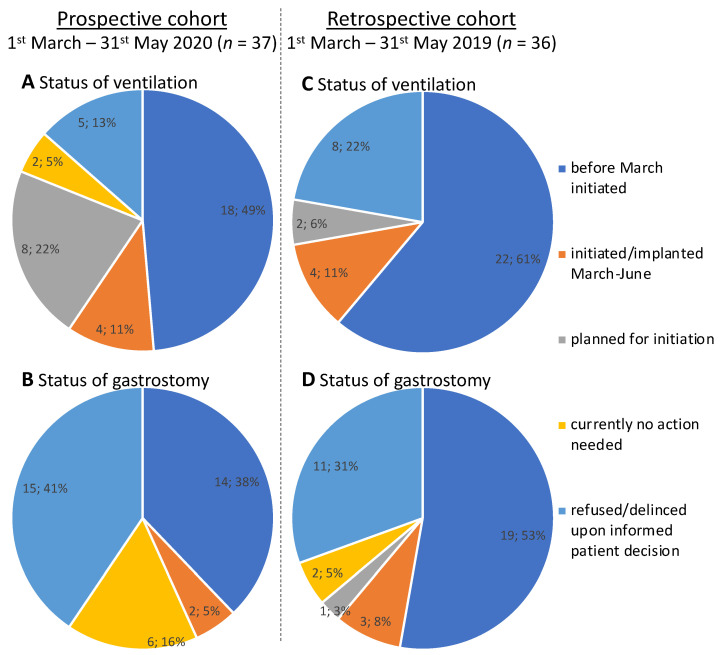
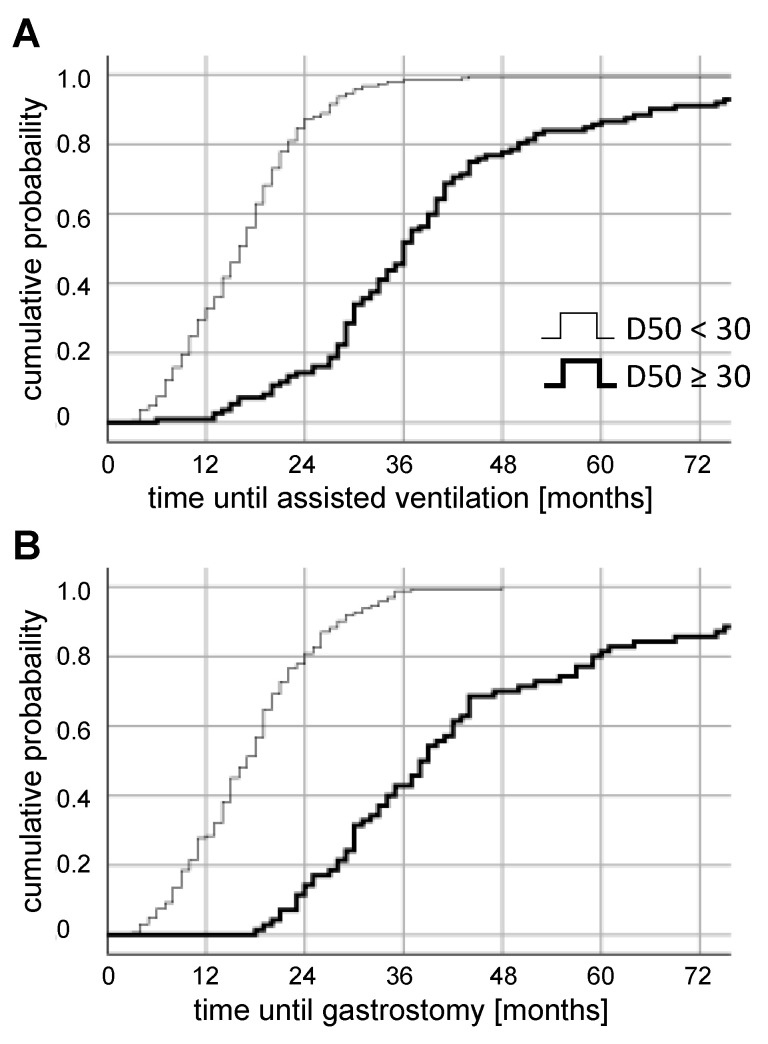
Amyotrophic lateral sclerosis (ALS) is a progressive neuromuscular disease, the management of which requires the continuous provision of multidisciplinary therapies. Owing to the novel coronavirus disease (COVID-19) pandemic, regular contact with ALS patients at our center was severely restricted and patient care was at risk by delay of supportive therapies. We established a triage system based on the D50 disease progression model and were thus able to identify a prospective cohort with high disease aggressiveness (D50 < 30). Thirty-seven patients with highly aggressive disease were actively offered follow-up, either via telephone or on-site, depending on their disease-specific needs and abilities. We describe here the procedures, obstacles, and results of these prescient efforts during the restrictions caused by COVID-19 in the period between March and June 2020. In conclusion, four patients with highly aggressive disease were initiated with non-invasive ventilation and two received a gastrostomy. We could show that a comparable amount of advanced care was induced in a retrospective cohort within a similar time period one year prior to the COVID-19 outbreak. Our workflow to identify high-risk patients via D50 model metrics can be easily implemented and integrated within existing centers. It helped to maintain a high quality of advanced care planning for our ALS patients.
Keywords: COVID-19; D50; SARS-CoV-2; amyotrophic lateral sclerosis; assisted ventilation; disease progression; gastrostomy; triage.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Westeneng H.J., Debray T.P.A., Visser A.E., Van Eijk R.P.A., Rooney J.P.K., Calvo A., Martin S., McDermott C.J., Thompson A.G., Pinto S., et al. Prognosis for patients with amyotrophic lateral sclerosis: Development and validation of a personalised prediction model. Lancet Neurol. 2018;17:423–433. doi: 10.1016/S1474-4422(18)30089-9. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
