

Invasive Hemodynamic Assessment and Classification of In-Hospital Mortality Risk Among Patients With Cardiogenic Shock
- PMID: 32900234
- PMCID: PMC10243474
- DOI: 10.1161/CIRCHEARTFAILURE.120.007099
Invasive Hemodynamic Assessment and Classification of In-Hospital Mortality Risk Among Patients With Cardiogenic Shock
Abstract
Background: Risk stratifying patients with cardiogenic shock (CS) is a major unmet need. The recently proposed Society for Cardiovascular Angiography and Interventions (SCAI) stages as an approach to identify patients at risk for in-hospital mortality remains under investigation. We studied the utility of the SCAI stages and further explored the impact of hemodynamic congestion on clinical outcomes.
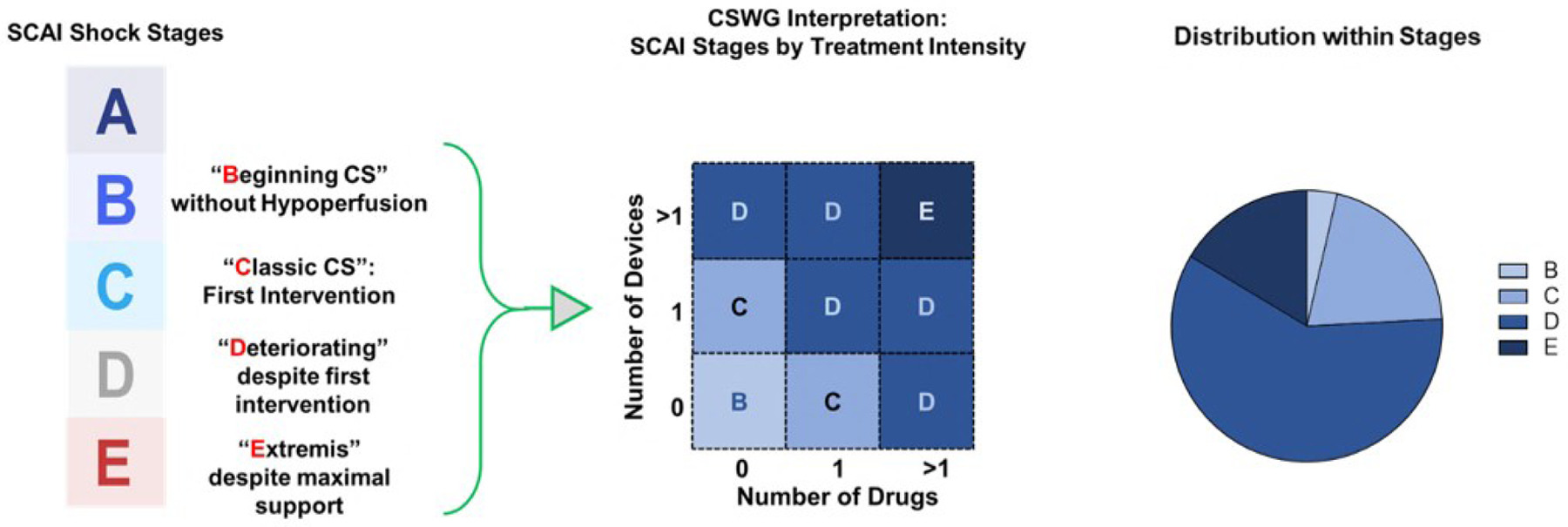
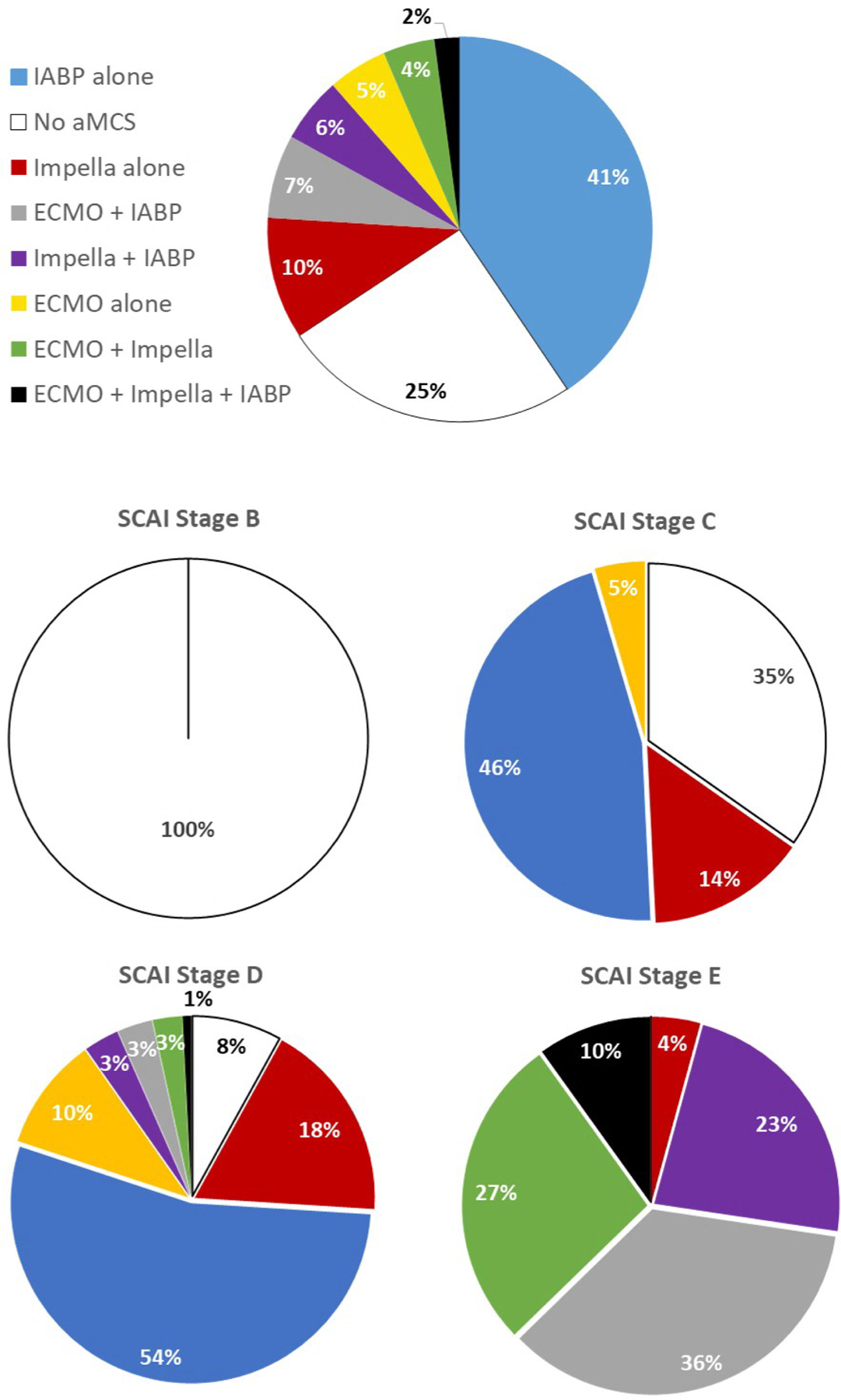
Methods: The CS Working Group registry includes patients with CS from 8 medical centers enrolled between 2016 and 2019. Patients were classified by the maximum SCAI stage (B-E) reached during their hospital stay according to drug and device utilization. In-hospital mortality was evaluated for association with SCAI stages and hemodynamic congestion.
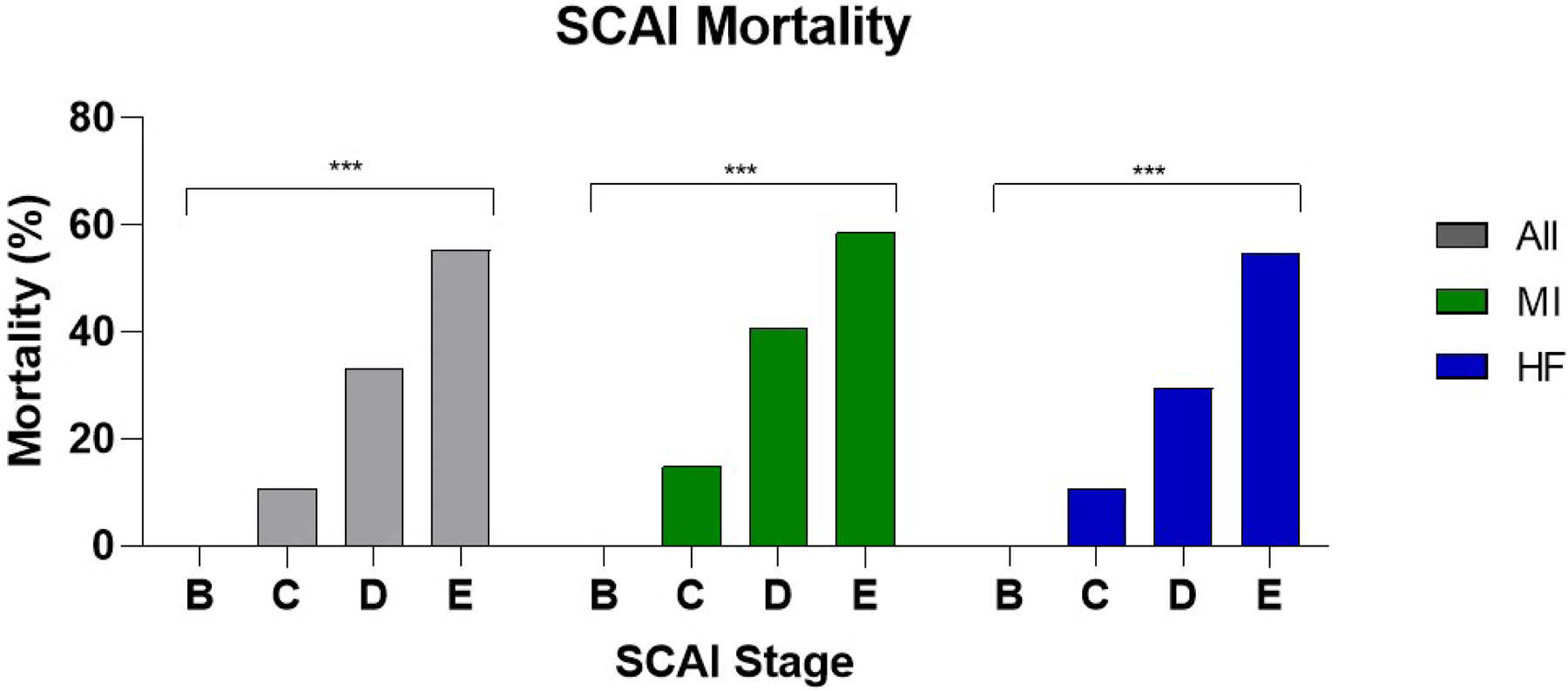
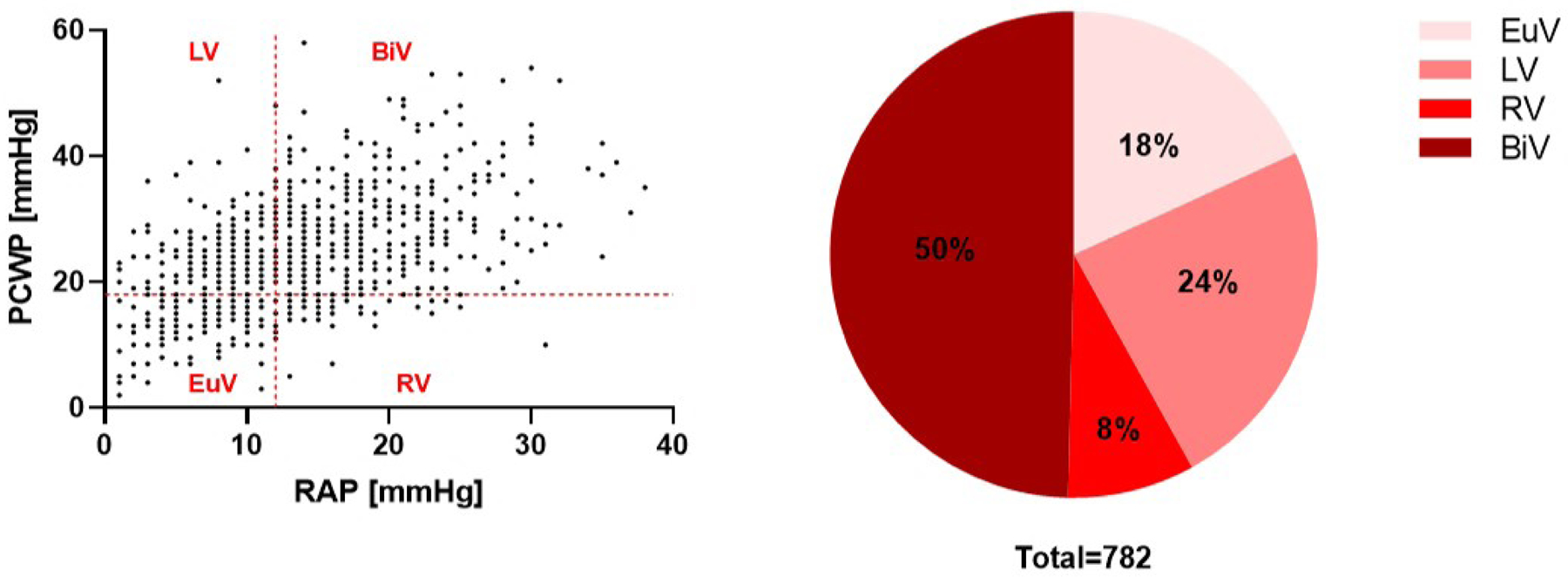
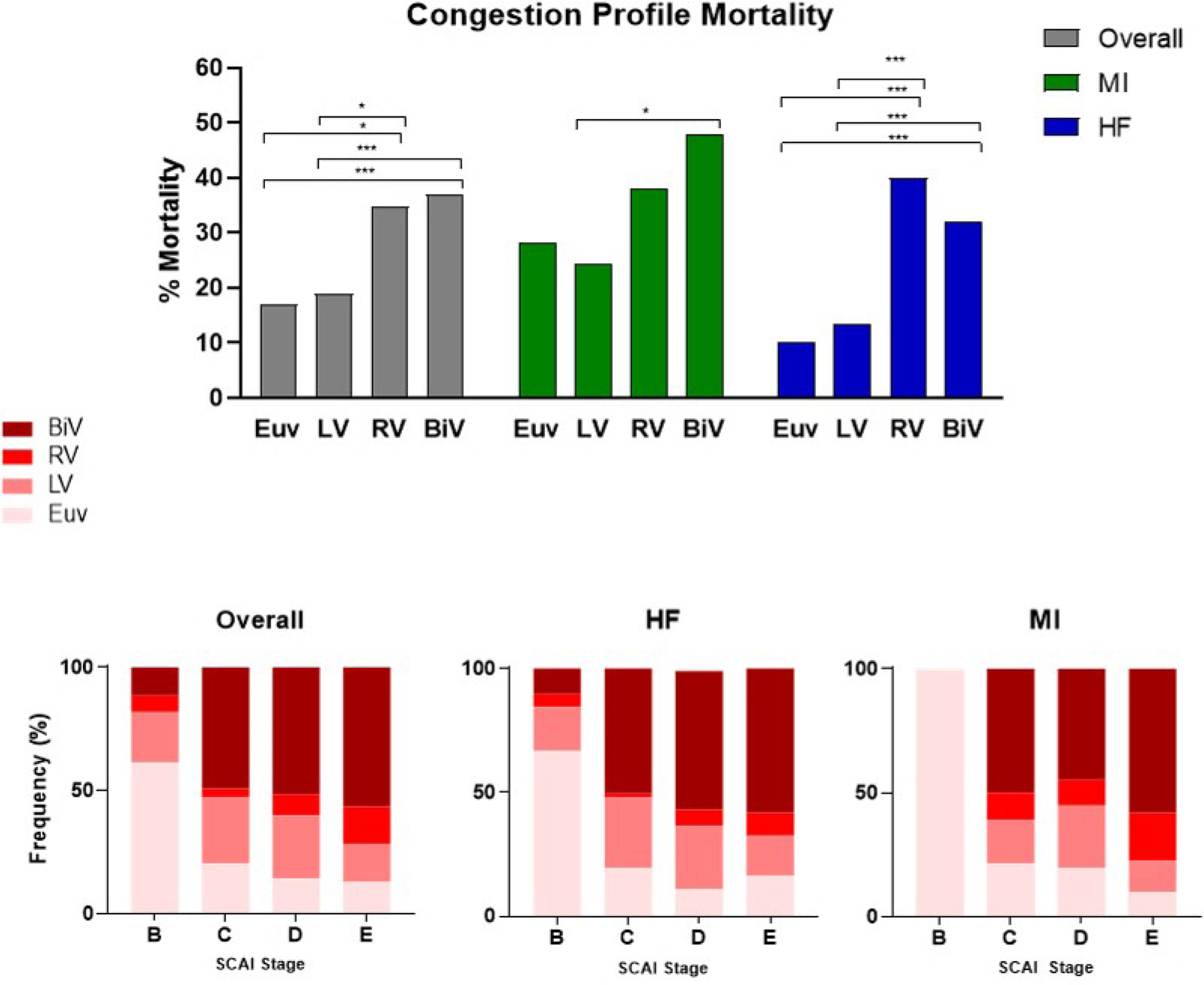
Results: Of the 1414 patients with CS, the majority were due to decompensated heart failure (50%) or myocardial infarction (MI; 35%). In-hospital mortality was 31% for the total cohort, but higher among patients with MI (41% versus 26%, MI versus heart failure, P<0.0001). Risk for in-hospital mortality was associated with increasing SCAI stage (odds ratio [95% CI], 3.25 [2.63-4.02]) in both MI and heart failure cohorts. Hemodynamic data was available in 1116 (79%) patients. Elevated biventricular filling pressures were common among patients with CS, and right atrial pressure was associated with increased mortality and higher SCAI Stage.
Conclusions: Our findings support an association between the proposed SCAI staging system and in-hospital mortality among patient with heart failure and MI. We further identify that venous congestion is common and identifies patients with CS at high risk for in-hospital mortality. These findings provide may inform future management protocols and clinical studies.
Keywords: cardiogenic shock; heart failure; hemodynamics; hospital mortality; myocardial infarction; right atrial pressure; ventricular congestion.
Conflict of interest statement
Disclosures
NKK receives consulting/speaker honoraria and institutional grant support from: Abbott Laboratories, Abiomed Inc., Boston Scientific, Medtronic, LivaNova, MDStart, and Precardia. JHM is a consultant for Abiomed Inc. JA is a consultant for Abbott Laboratories, Abiomed Inc. DB reports an unrestricted, educational grant from Abiomed Inc. to Cardiovascular Research Foundation. SSS is a consultant for Abiomed Inc. (Critical Care Advisory Board). WON receives consulting/speaker honoraria from Abiomed Inc. KLT, EZ, MA, ARG, JHM, CM, KM, SN, LJ, MLE, CDD, DW, EV, NMH, JLH have nothing to disclose.
Figures
Comment in
-
Understanding Cardiogenic Shock Severity and Mortality Risk Assessment.Circ Heart Fail. 2020 Sep;13(9):e007568. doi: 10.1161/CIRCHEARTFAILURE.120.007568. Epub 2020 Sep 9. Circ Heart Fail. 2020. PMID: 32900232 No abstract available.
References
-
- Kolte D, Khera S, Aronow WS, Mujib M, Palaniswamy C, Sule S, Jain D, Gotsis W, Ahmed A, Frishman WH and Fonarow GC. Trends in incidence, management, and outcomes of cardiogenic shock complicating ST-elevation myocardial infarction in the United States. J Am Heart Assoc 2014;3:e000590. - PMC - PubMed
-
- van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, Thiele H, Washam JB, Cohen MG, American Heart Association Council on Clinical C, Council on C, Stroke N, Council on Quality of C, Outcomes R and Mission L. Contemporary Management of Cardiogenic Shock: A Scientific Statement From the American Heart Association. Circulation 2017;136:e232–e268. - PubMed
-
- Goldberg RJ, Makam RC, Yarzebski J, McManus DD, Lessard D and Gore JM. Decade-Long Trends (2001–2011) in the Incidence and Hospital Death Rates Associated with the In-Hospital Development of Cardiogenic Shock after Acute Myocardial Infarction. Circ Cardiovasc Qual Outcomes 2016;9:117–25. - PMC - PubMed
-
- Becher PM, Schrage B, Sinning CR, Schmack B, Fluschnik N, Schwarzl M, Waldeyer C, Lindner D, Seiffert M, Neumann JT, Bernhardt AM, Zeymer U, Thiele H, Reichenspurner H, Blankenberg S, Twerenbold R and Westermann D. Venoarterial Extracorporeal Membrane Oxygenation for Cardiopulmonary Support. Circulation 2018;138:2298–2300. - PubMed
-
- Thiele H, Zeymer U, Neumann FJ, Ferenc M, Olbrich HG, Hausleiter J, Richardt G, Hennersdorf M, Empen K, Fuernau G, Desch S, Eitel I, Hambrecht R, Fuhrmann J, Bohm M, Ebelt H, Schneider S, Schuler G, Werdan K and Investigators I-SIT. Intraaortic balloon support for myocardial infarction with cardiogenic shock. N Engl J Med 2012;367:1287–96. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
