

A pilot study of high frequency accelerometry-based sedation and agitation monitoring in critically ill patients
- PMID: 32900331
- PMCID: PMC10699079
- DOI: 10.1016/S1441-2772(23)00392-7
A pilot study of high frequency accelerometry-based sedation and agitation monitoring in critically ill patients
Abstract
Objective: The degree of sedation or agitation in critically ill patients is typically assessed with the Richmond Agitation and Sedation Scale (RASS). However, this approach is intermittent and subject to unrecognised variation between assessments. High frequency accelerometry may assist in achieving a quantitative and continuous assessment of sedation while heralding imminent agitation.
Design: We undertook a prospective, observational pilot study.
Setting: An adult tertiary intensive care unit in Melbourne, Australia.
Participants: 20 patients with an admission diagnosis of trauma.
Main outcome measures: Accelerometers were applied to patients' wrists and used to continuously record patient movement. Video data of patient behaviour were simultaneously collected, and observers blinded to accelerometry data were adjudicated the RASS score every 30 seconds. Exploratory analyses were undertaken.
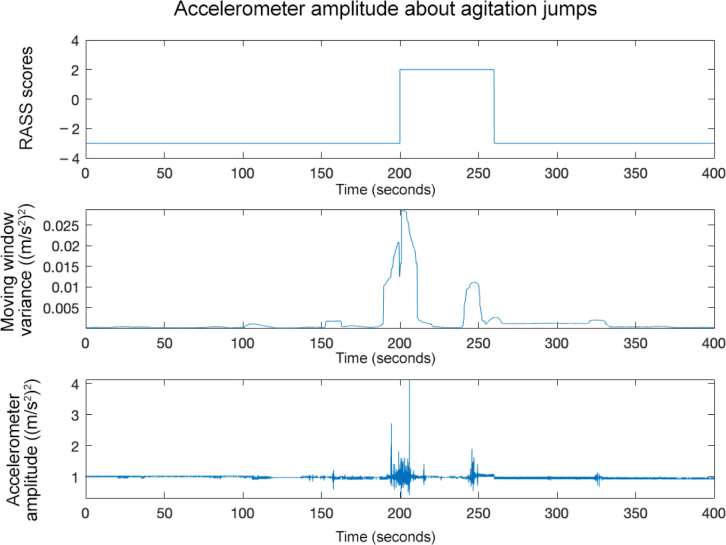
Results: Patients were enrolled for a median duration of 9.7 hours (interquartile range [IQR], 0-22.8) and a total of 160 hours. These patients had a median RASS score of 0 (IQR, -4 to 0). A 2-minute moving window of amplitude variance was seen to reflect contemporaneous fluctuations in motor activity and was proportional to the RASS score. Furthermore, the moving window of amplitude variance was observed to spike immediately before ≥ 2 point increases in the RASS score.
Conclusions: We describe a novel approach to the analysis of wrist accelerometry data in critically ill patients. This technique not only appears to provide novel and continuous information about the depth of sedation or degree of agitation, it is also notable in its aptitude to anticipate impending transitions to higher RASS values.
Conflict of interest statement
None declared.
Figures




References
-
- Kress J.P., Pohlman A.S., O’Connor M.F., Hall J.B. Daily interruption of sedative infusions in critically ill patients undergoing mechanical ventilation. New Engl J Med. 2000;342:1471–1477. - PubMed
-
- De Jonghe B., Bastuji-Garin S., Fangio P., et al. Sedation algorithm in critically ill patients without acute brain injury. Crit Care Med. 2005;33:120–127. - PubMed
-
- Strøm T., Martinussen T., Toft P. A protocol of no sedation for critically ill patients receiving mechanical ventilation: a randomised trial. Lancet. 2010;375:475–480. - PubMed
-
- Girard T.D., Kress J.P., Fuchs B.D., et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008;371:126–134. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
