

Invasive and Non-Invasive Ventilation in Patients With COVID-19
- PMID: 32900426
- PMCID: PMC7658682
- DOI: 10.3238/arztebl.2020.0528
Invasive and Non-Invasive Ventilation in Patients With COVID-19
Abstract
Background: The reported high mortality of COVID-19 patients in intensive care has given rise to a debate over whether patients with this disease are being intubated too soon and might instead benefit from more non-invasive ventilation.
Methods: This review is based on articles published up to 12 June 2020 that were retrieved by a selective literature search on the topic of invasive and non-invasive ventilation for respiratory failure in COVID-19. Guideline recommendations and study data on patients with respiratory failure in settings other than COVID-19 are also considered, as are the current figures of the intensive care registry of the German Interdisciplinary Association for Intensive Care and Emergency Medicine (Deutsche Interdisziplinäre Vereinigung für Intensiv- und Notfallmedizin).
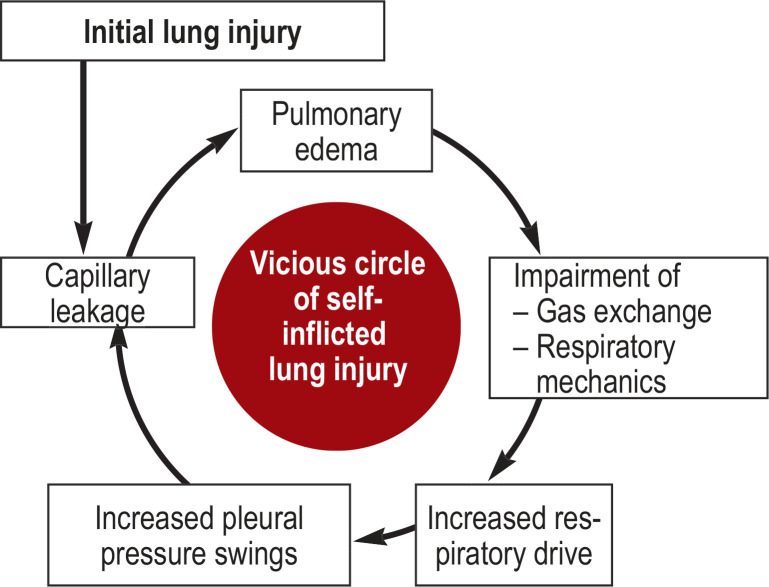
Results: The high mortality figures among patients receiving invasive ventilation that have been reported in studies from abroad cannot be uncritically applied to the current situation in Germany. Study data on ventilation specifically in COVID-19 patients would be needed to do justice to the special pathophysiology of this disease, but such data are lacking. Being intubated too early is evidently associated with risks for the patient, but being intubated too late is as well. A particularly im - portant consideration is the potential harm associated with prolonged spontaneous breathing, with or without non-invasive assistance, as any increase in respiratory work can seriously worsen respiratory failure. On the other hand, it is clearly unacceptable to intubate patients too early merely out of concern that the medical staff might become infected with COVID-19 if they were ventilated non-invasively.
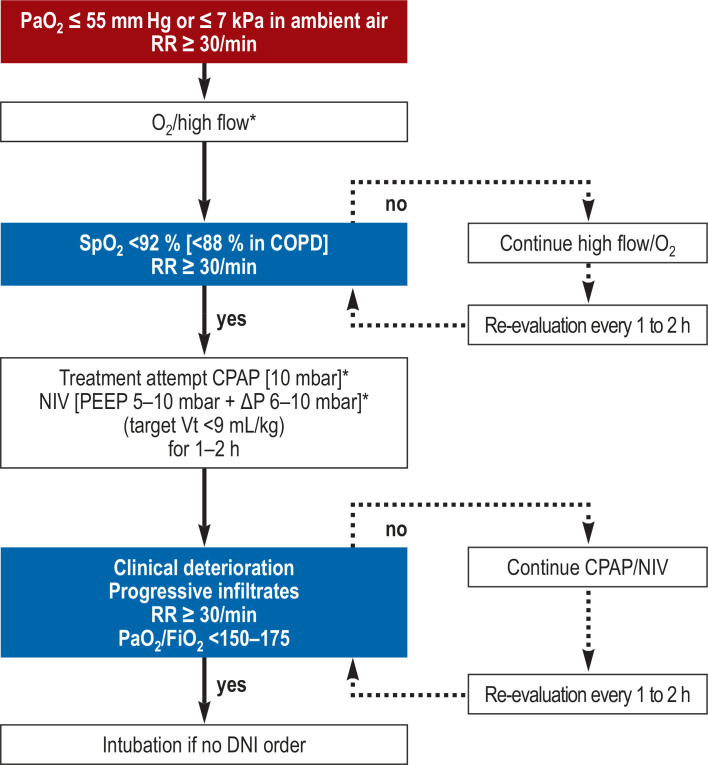
Conclusion: Nasal high flow, non-invasive ventilation, and invasive ventilation with intubation should be carried out in a stepwise treatment strategy, under appropriate intensive-care monitoring and with the observance of all relevant anti-infectious precautions. Germany is better prepared that other countries to provide COVID-19 patients with appropriate respiratory care, in view of the high per capita density of intensive-care beds and the availability of a nationwide, interdisciplinary intensive care registry for the guidance and coordination of intensive care in patients who need it.
Figures
References
-
- Soldt R. Es wird zu häufig intubiert Frankfurter Allgemeine Zeitung (published on 7 April 2020) www.faz.net/aktuell/gesellschaft/gesundheit/coronavirus/beatmung-beim-co... (last accessed on 29 June 2020)
-
- Voshaar T, Dellweg D, Hetzel M. published by Verband Pneumologischer Kliniken: Empfehlung zur Behandlung respiratorischer Komplikationen bei akuter Virusinfektion außerhalb der Intensivstation. www.vpneumo.de/fileadmin/pdf/VPK_Empfehlung_neu_21.03.2020.pdf (last accessed on 29 June 2020)
-
- Westhoff M, Schönhofer B, Neumann P, et al. S3 Leitlinien: Nicht-invasive Beatmung als Therapie der akuten respiratorischen Insuffizienz. Pneumologie. 2015;69:719–756. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical