

Novel role of lncRNA CHRF in cisplatin resistance of ovarian cancer is mediated by miR-10b induced EMT and STAT3 signaling
- PMID: 32901049
- PMCID: PMC7478977
- DOI: 10.1038/s41598-020-71153-0
Novel role of lncRNA CHRF in cisplatin resistance of ovarian cancer is mediated by miR-10b induced EMT and STAT3 signaling
Abstract
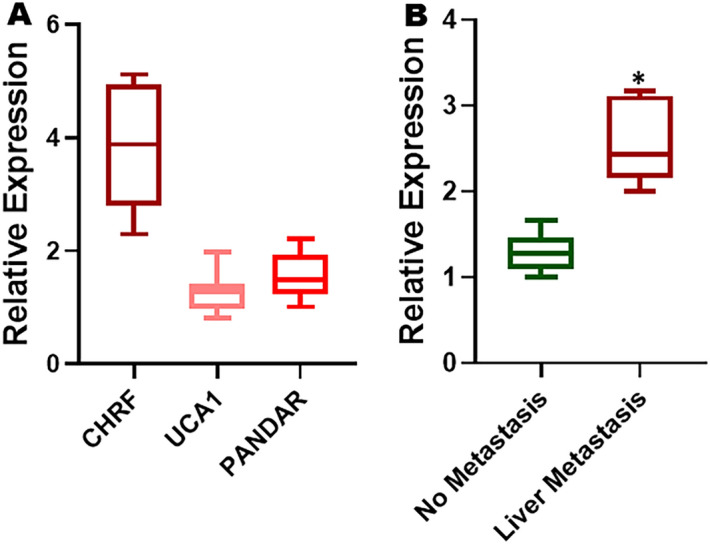
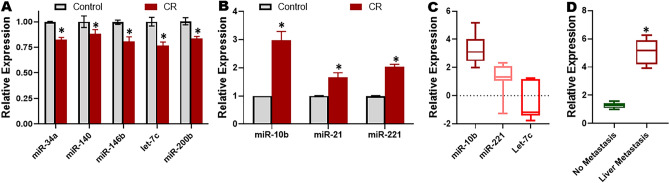
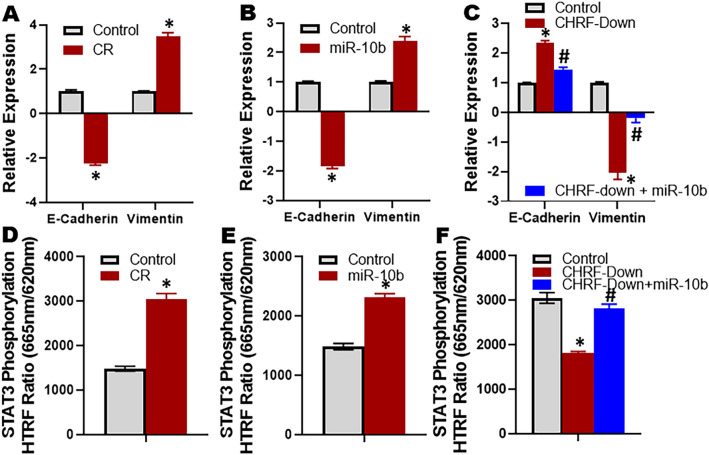
Ovarian Cancer (OC) is a highly lethal gynecological cancer which often progresses through acquired resistance against the administered therapy. Cisplatin is a common therapeutic for the treatment of OC patients and therefore it is critical to understand the mechanisms of resistance against this drug. We studied a paired cell line consisting of parental and cisplatin resistant (CR) derivative ES2 OC cells, and found a number of dysregulated lncRNAs, with CHRF being the most significantly upregulated lncRNA in CR ES2 cells. The findings corroborated in human patient samples and CHRF was significantly elevated in OC patients with resistant disease. CHRF was also found to be elevated in patients with liver metastasis. miR-10b was found to be mechanistically involved in CHRF mediated cisplatin resistance. It induced resistance in not only ES2 but also OVCAR and SKOV3 OC cells. Induction of epithelial-to-mesenchymal-transition (EMT) and activation of STAT3 signaling were determined to be the mechanisms underlying the CHRF-miR-10b axis-mediated cisplatin resistance. Down-regulation of CHRF reversed EMT, STAT3 activation and the resulting cisplatin resistance, which could be attenuated by miR-10b. The results were also validated in an in vivo cisplatin resistance model wherein CR cells were associated with increased tumor burden, CHRF downregulation associated with decreased tumor burden and miR-10b again attenuated the CHRF downregulation effects. Our results support a novel role of lncRNA CHRF in cisplatin resistance of OC and establish CHRF-miR-10b signaling as a putative therapeutic target for sensitizing resistant OC cells.
Conflict of interest statement
The authors declare no competing interests.
Figures



Similar articles
-
IL-6R/STAT3/miR-204 feedback loop contributes to cisplatin resistance of epithelial ovarian cancer cells.Oncotarget. 2017 Jun 13;8(24):39154-39166. doi: 10.18632/oncotarget.16610. Oncotarget. 2017. PMID: 28388577 Free PMC article.
-
MicroRNA-302 represses epithelial-mesenchymal transition and cisplatin resistance by regulating ATAD2 in ovarian carcinoma.Exp Cell Res. 2020 Nov 1;396(1):112241. doi: 10.1016/j.yexcr.2020.112241. Epub 2020 Aug 21. Exp Cell Res. 2020. PMID: 32835657
-
Long Non-coding RNA CCAT1 Sponges miR-454 to Promote Chemoresistance of Ovarian Cancer Cells to Cisplatin by Regulation of Surviving.Cancer Res Treat. 2020 Jul;52(3):798-814. doi: 10.4143/crt.2019.498. Epub 2020 Mar 3. Cancer Res Treat. 2020. PMID: 32124583 Free PMC article.
-
The long noncoding RNA CRAL reverses cisplatin resistance via the miR-505/CYLD/AKT axis in human gastric cancer cells.RNA Biol. 2020 Nov;17(11):1576-1589. doi: 10.1080/15476286.2019.1709296. Epub 2020 Jan 7. RNA Biol. 2020. PMID: 31885317 Free PMC article. Review.
-
Evaluation of Long Non-coding RNA (LncRNA) in the Pathogenesis of Chemotherapy Resistance in Cervical Cancer: Diagnostic and Prognostic Approach.Mol Biotechnol. 2024 Oct;66(10):2751-2768. doi: 10.1007/s12033-023-00909-6. Epub 2023 Oct 7. Mol Biotechnol. 2024. PMID: 37804407 Review.
Cited by
-
IL-1β-Triggered Long Non-coding RNA CHRF Induces Non-Small Cell Lung Cancer by Modulating the microRNA-489/Myd88 Axis.J Cancer. 2022 May 16;13(8):2620-2630. doi: 10.7150/jca.63256. eCollection 2022. J Cancer. 2022. PMID: 35711847 Free PMC article.
-
Role of STAT3 in cancer cell epithelial‑mesenchymal transition (Review).Int J Oncol. 2024 May;64(5):48. doi: 10.3892/ijo.2024.5636. Epub 2024 Mar 15. Int J Oncol. 2024. PMID: 38488027 Free PMC article. Review.
-
Chemotherapy-induced metastasis: molecular mechanisms and clinical therapies.Acta Pharmacol Sin. 2023 Sep;44(9):1725-1736. doi: 10.1038/s41401-023-01093-8. Epub 2023 May 11. Acta Pharmacol Sin. 2023. PMID: 37169853 Free PMC article. Review.
-
The Emerging Role of Non-coding RNAs in Drug Resistance of Ovarian Cancer.Front Genet. 2021 Aug 20;12:693259. doi: 10.3389/fgene.2021.693259. eCollection 2021. Front Genet. 2021. PMID: 34512721 Free PMC article. Review.
-
Identification of a Novel Immune-Related lncRNA CTD-2288O8.1 Regulating Cisplatin Resistance in Ovarian Cancer Based on Integrated Analysis.Front Genet. 2022 Feb 14;13:814291. doi: 10.3389/fgene.2022.814291. eCollection 2022. Front Genet. 2022. PMID: 35237300 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
