

Conversion from mini bypass to laparoscopic Roux en Y gastric bypass in an emergency setting: Case report and literature review
- PMID: 32901216
- PMCID: PMC7457964
- DOI: 10.1016/j.ijscr.2020.08.032
Conversion from mini bypass to laparoscopic Roux en Y gastric bypass in an emergency setting: Case report and literature review
Abstract
Introduction: It has been demonstrated that certain technique endpoints are key to the success for the OAGB and RYGB procedures but only a few texts in which post-operative complications are documented.
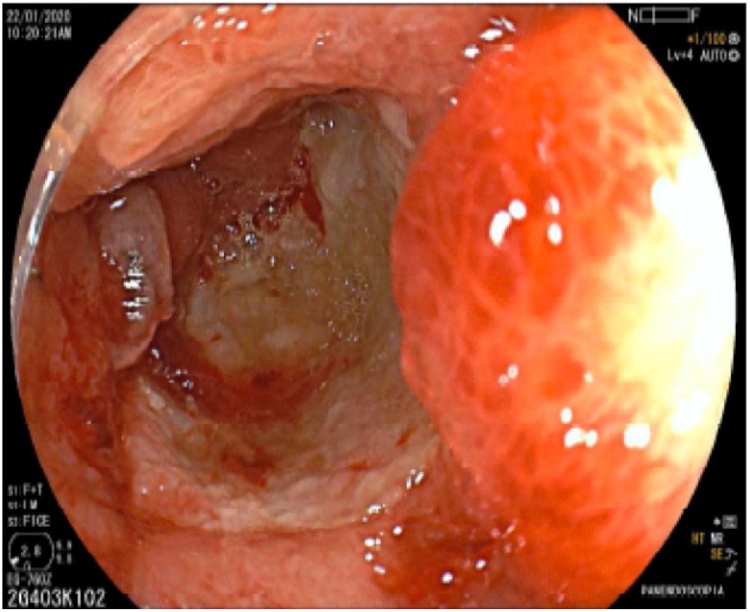
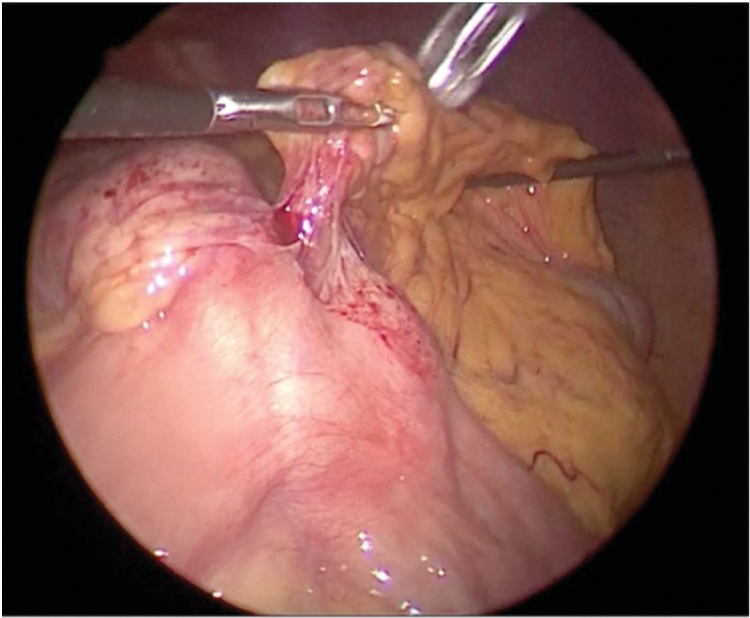
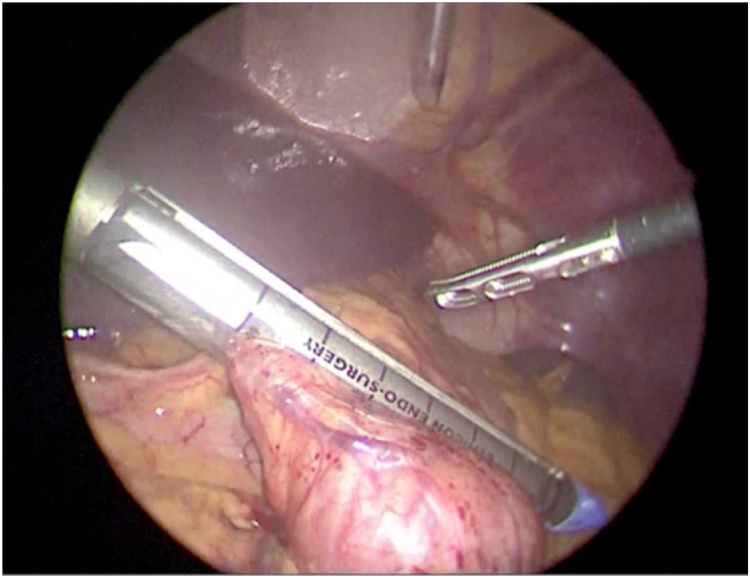
Presentation of case: 42-year-old male patient admitted to the emergency department for presenting abdominal pain located in the epigastrium for 4 days, melenic evacuations and syncope on one occasion. Two years prior to admission, the patient underwent a single anastomosis bypass for grade III obesity.Gastric bypass mini revision surgery was performed an antecolic and antegastric gastrointestinal anastomosis was made with a 3 cm latero-lateral anastomosis; an intestinal-intestinal anastomosis was performed 60 cm from the gastric anastomosis. The length of the biliopancreatic loop (120 cm) and the feeding loop (60 cm) are reviewed.
Discussion: Performing an "en bloc" resection of the anastomosis is essential since bile reflux is one of the irritation mechanisms of the anastomosis but not the only one. The size of the gastric pouch directly influences the frequency of marginal ulcers, so during the OAGBP revision, the gastro-jejunal junction must be resected to remodel it, reducing the size of the gastric reservoir that allows to perform the new anastomosis in less inflamed tissue. Roux-en-Y reconstruction should be performed once the length of the biliopancreatic loop is verified and it does not exceed 150 cm and a short alimentary loop to avoid nutritional complications.Complications arising from bariatric procedures are varied, infrequent in well-trained surgeons, but severe in inexpert hands, leading to an increase in mortality rates.
Conclusions: We propose the laparoscopic conversion of OAGB to RYGB as a safe method, and feasible in hemodynamically unstable patients.
Keywords: Anastomoses; Bariatric surgery; Complications; RYGB.
© 2020 The Authors.
Figures



Similar articles
-
Conversion of One Anastomosis Gastric Bypass (OAGB) to Roux-en-Y Gastric Bypass (RYGB) for Biliary Reflux Resistant to Medical Treatment: Lessons Learned from a Retrospective Series of 2780 Consecutive Patients Undergoing OAGB.Obes Surg. 2020 Jun;30(6):2093-2098. doi: 10.1007/s11695-020-04460-0. Obes Surg. 2020. PMID: 32052289
-
Laparoscopic Conversion of One Anastomosis Gastric Bypass to Roux-en-Y Gastric Bypass for Chronic Bile Reflux.Obes Surg. 2016 Mar;26(3):701-3. doi: 10.1007/s11695-015-2017-8. Obes Surg. 2016. PMID: 26746224
-
Roux en Y gastric bypass and iterative intussusception at the jejuno-jejunal anastomosis: Conversion into one anastomosis gastric bypass (with video) - A case report.Int J Surg Case Rep. 2024 Feb;115:109244. doi: 10.1016/j.ijscr.2024.109244. Epub 2024 Jan 10. Int J Surg Case Rep. 2024. PMID: 38215577 Free PMC article.
-
Randomized Controlled Trial of One Anastomosis Gastric Bypass Versus Roux-En-Y Gastric Bypass for Obesity: Comparison of the YOMEGA and Taiwan Studies.Obes Surg. 2019 Sep;29(9):3047-3053. doi: 10.1007/s11695-019-04065-2. Obes Surg. 2019. PMID: 31290104 Review.
-
Anastomotic Gastro-Jejunal Ulcer Perforation Following One Anastomosis Gastric Bypass: Clinical Presentation and Options of Management-Case Series and Review of Literature.Obes Surg. 2020 Jun;30(6):2423-2428. doi: 10.1007/s11695-020-04423-5. Obes Surg. 2020. PMID: 32062846 Review.
Cited by
-
Emergent conversion from single-anastomosis gastric bypass to Roux-en-Y gastric bypass with subsequent obstruction of entero-enteric anastomosis by ascaris.J Surg Case Rep. 2023 Aug 22;2023(8):rjad428. doi: 10.1093/jscr/rjad428. eCollection 2023 Aug. J Surg Case Rep. 2023. PMID: 37614466 Free PMC article.
-
Bile reflux after one anastomosis gastric bypass surgery: A review study.Ann Med Surg (Lond). 2021 Mar 26;64:102248. doi: 10.1016/j.amsu.2021.102248. eCollection 2021 Apr. Ann Med Surg (Lond). 2021. PMID: 33868682 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
