

Use of nasal high flow oxygen during acute respiratory failure
- PMID: 32901374
- PMCID: PMC7478440
- DOI: 10.1007/s00134-020-06228-7
Use of nasal high flow oxygen during acute respiratory failure
Abstract
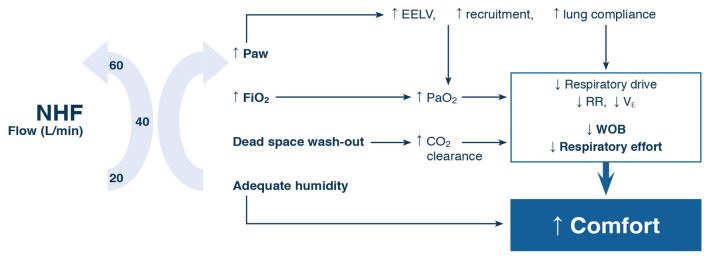
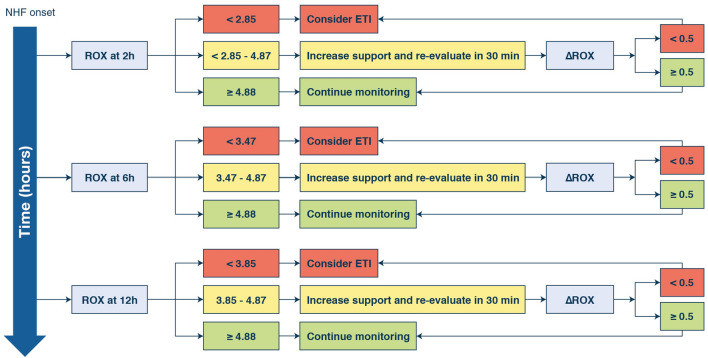
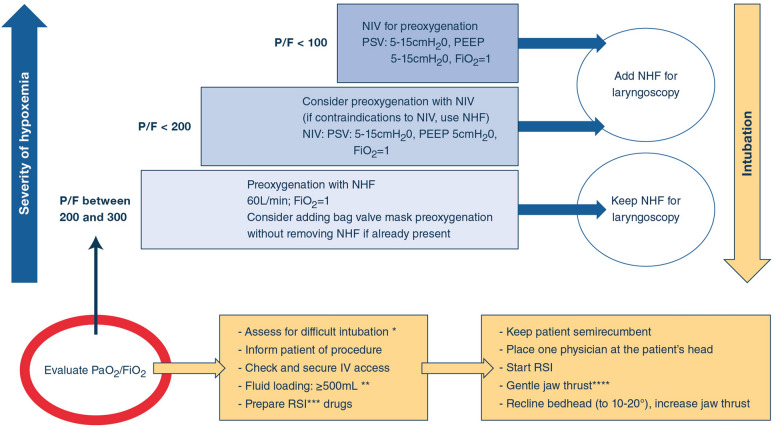
Nasal high flow (NHF) has gained popularity among intensivists to manage patients with acute respiratory failure. An important literature has accompanied this evolution. In this review, an international panel of experts assessed potential benefits of NHF in different areas of acute respiratory failure management. Analyses of the physiological effects of NHF indicate flow-dependent improvement in various respiratory function parameters. These beneficial effects allow some patients with severe acute hypoxemic respiratory failure to avoid intubation and improve their outcome. They require close monitoring to not delay intubation. Such a delay may worsen outcome. The ROX index may help clinicians decide when to intubate. In immunocompromised patients, NHF reduces the need for intubation but does not impact mortality. Beneficial physiological effects of NHF have also been reported in patients with chronic respiratory failure, suggesting a possible indication in acute hypercapnic respiratory failure. When intubation is required, NHF can be used to pre-oxygenate patients either alone or in combination with non-invasive ventilation (NIV). Similarly, NHF reduces reintubation alone in low-risk patients and in combination with NIV in high-risk patients. NHF may be used in the emergency department in patients who would not be offered intubation and can be better tolerated than NIV.
Keywords: ARDS; Acute respiratory failure; High flow oxygen; Intubation; Nasal canula; Palliative care.
Conflict of interest statement
JDR received travel expenses and accommodation coverage from Fisher&Paykel Healthcare to attend scientific meetings. Fisher&Paykel Healthcare provided support for the ongoing High Flow ACRF trial (NCT03406572) but took no part in design or conduct of the study. OR received speaker fees from Air Liquide. His institution received consultancy fees from Hamilton Medical. VL has no conflict of interest to declare concerning this topic. JB received travel expenses, lecture fees and accommodation coverage from TNI medical AG and Fisher & Paykel Healthcare. TNI medical AG provided support for several NHF trials. AC’s employer, on her behalf, has received travel expenses, lecture fees and accommodation from Fisher & Paykel Healthcare to attend scientific meetings. Fisher & Paykel Healthcare has also provided an unrestricted grant to support investigator driven research, but has had no part in study design, conduct, analysis or reporting of the studies. PJ received competitive grant funding from the A + Trust (4926) and Greenlane Research and Education Fund (12/15/4086) for the HOTER RCT (ACTRN12610000960411) on HFNO in the ED. F&P Healthcare provided equipment for the HOTER RCT for which PJ was the principal investigator, but took no part in design, conduct, analysis or reporting of the study. PJ has no other personal financial or professional to declare. BJK: has no conflict of interest to declare. FL: Fisher&Paykel Healthcare provided support for the development of an application VentilO on optimization of protective mechanical ventilation. SN: Fisher&Paykel Healthcare provided support for the study # NCT03759457. NR received travel expenses and lecture fees from Fisher&Paykel Healthcare. GS: Fisher&Paykel Healthcare provided support for the study # NCT03965832 for which GS is the principal investigator. SJ received personal fees as consultant from Fisher-Paykel. GH received travel expenses coverage and lecture fees from Fisher&Paykel.
Figures
References
-
- Delorme M, Bouchard P-A, Simon M, et al. Effects of high-flow nasal cannula on the work of breathing in patients recovering from acute respiratory failure. Crit Care Med. 2017;45:1981–1988. - PubMed
-
- Mauri T, Alban L, Turrini C, et al. Optimum support by high-flow nasal cannula in acute hypoxemic respiratory failure: effects of increasing flow rates. Intensive Care Med. 2017;43:1453–1463. - PubMed
-
- Mauri T, Turrini C, Eronia N, et al. Physiologic effects of high-flow nasal cannula in acute hypoxemic respiratory failure. Am J Respir Crit Care Med. 2017;195:1207–1215. - PubMed
-
- Corley A, Caruana LR, Barnett AG, et al. Oxygen delivery through high-flow nasal cannulae increase end-expiratory lung volume and reduce respiratory rate in post-cardiac surgical patients. Br J Anaesth. 2011;107:998–1004. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
