

The Role of Imaging in Current Treatment Strategies for Pancreatic Adenocarcinoma
- PMID: 32901458
- PMCID: PMC7772381
- DOI: 10.3348/kjr.2019.0862
The Role of Imaging in Current Treatment Strategies for Pancreatic Adenocarcinoma
Abstract
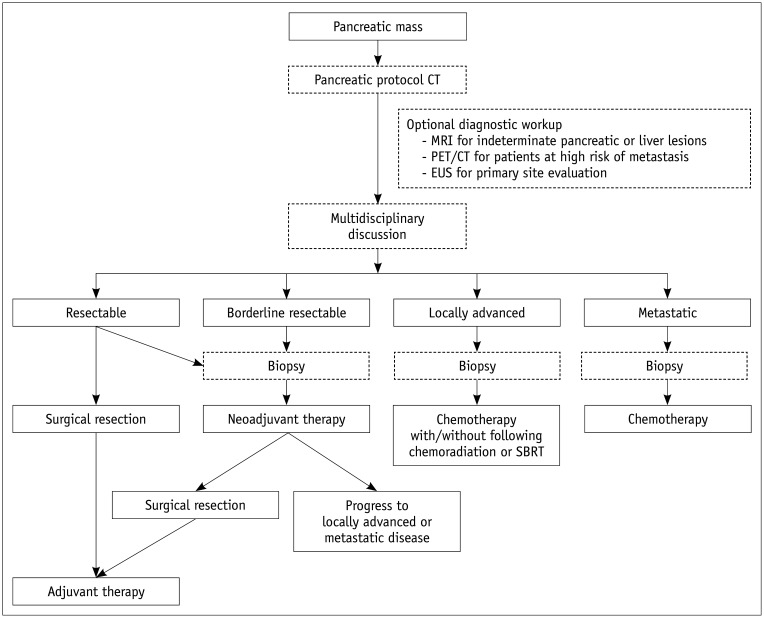
In pancreatic cancer, imaging plays an essential role in surveillance, diagnosis, resectability evaluation, and treatment response evaluation. Pancreatic cancer surveillance in high-risk individuals has been attempted using endoscopic ultrasound (EUS) or magnetic resonance imaging (MRI). Imaging diagnosis and resectability evaluation are the most important factors influencing treatment decisions, where computed tomography (CT) is the preferred modality. EUS, MRI, and positron emission tomography play a complementary role to CT. Treatment response evaluation is of increasing clinical importance, especially in patients undergoing neoadjuvant therapy. This review aimed to comprehensively review the role of imaging in relation to the current treatment strategy for pancreatic cancer, including surveillance, diagnosis, evaluation of resectability and treatment response, and prediction of prognosis.
Keywords: Diagnosis; Imaging; Pancreatic cancer; Prognosis; Resectability; Response evaluation.
Copyright © 2021 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. - PubMed
-
- Malvezzi M, Carioli G, Bertuccio P, Boffetta P, Levi F, La Vecchia C, et al. European cancer mortality predictions for the year 2019 with focus on breast cancer. Ann Oncol. 2019;30:781–787. - PubMed
-
- Ferlay J, Colombet M, Soerjomataram I, Dyba T, Randi G, Bettio M, et al. Cancer incidence and mortality patterns in Eeurope: estimates for 40 countries and 25 major cancers in 2018. Eur J Cancer. 2018;103:356–387. - PubMed
-
- Ducreux M, Cuhna AS, Caramella C, Hollebecque A, Burtin P, Goéré D, et al. Cancer of the pancreas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26 Suppl 5:v56–v68. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
