

Prognostic assessment of resected colorectal liver metastases integrating pathological features, RAS mutation and Immunoscore
- PMID: 32902189
- PMCID: PMC7737782
- DOI: 10.1002/cjp2.178
Prognostic assessment of resected colorectal liver metastases integrating pathological features, RAS mutation and Immunoscore
Abstract
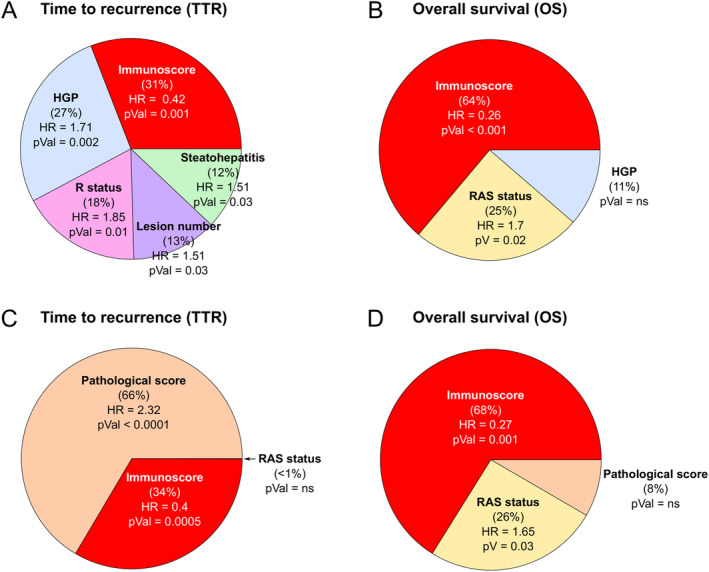
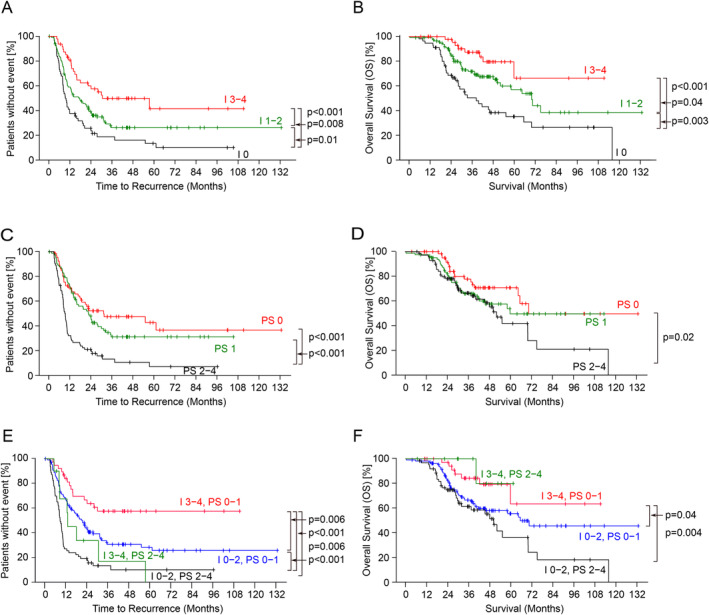
Surgical resection of colorectal liver metastases combined with systemic treatment aims to maximize patient survival. However, recurrence rates are very high postsurgery. In order to assess patient prognosis after metastasis resection, we evaluated the main patho-molecular and immune parameters of all surgical specimens. Two hundred twenty-one patients who underwent, after different preoperative treatment, curative resection of 582 metastases were analyzed. Clinicopathological parameters, RAS tumor mutation, and the consensus Immunoscore (I) were assessed for all patients. Overall survival (OS) and time to relapse (TTR) were estimated using the Kaplan-Meier method and compared by log-rank tests. Cox proportional hazard models were used for uni- and multivariate analysis. Immunoscore and clinicopathological parameters (number of metastases, surgical margin, histopathological growth pattern, and steatohepatitis) were associated with relapse in multivariate analysis. Overall, pathological score (PS) that combines relevant clinicopathological factors for relapse, and I, were prognostic for TTR (2-year TTR rate PS 0-1: 49.8.% (95% CI: 42.2-58.8) versus PS 2-4: 20.9% (95% CI: 13.4-32.8), hazard ratio (HR) = 2.54 (95% CI: 1.82-3.53), p < 0.0000; and 2-year TTR rate I 0: 25.7% (95% CI: 16.3-40.5) versus I 3-4: 60% (95% CI: 47.2-76.3), HR = 2.87 (95% CI: 1.73-4.75), p = 0.0000). Immunoscore was also prognostic for OS (HR [I 3-4 versus I 0] = 4.25, 95% CI: 1.95-9.23; p = 0.0001). Immunoscore (HR [I 3-4 versus I 0] = 0.27, 95% CI: 0.12-0.58; p = 0.0009) and RAS mutation (HR [mutated versus WT] = 1.66, 95% CI: 1.06-2.58; p = 0.0265) were significant for OS. In conclusion, PS including relevant clinicopathological parameters and Immunoscore permit stratification of stage IV colorectal cancer patient prognosis in terms of TTR and identify patients with higher risk of recurrence. Immunoscore remains the major prognostic factor for OS.
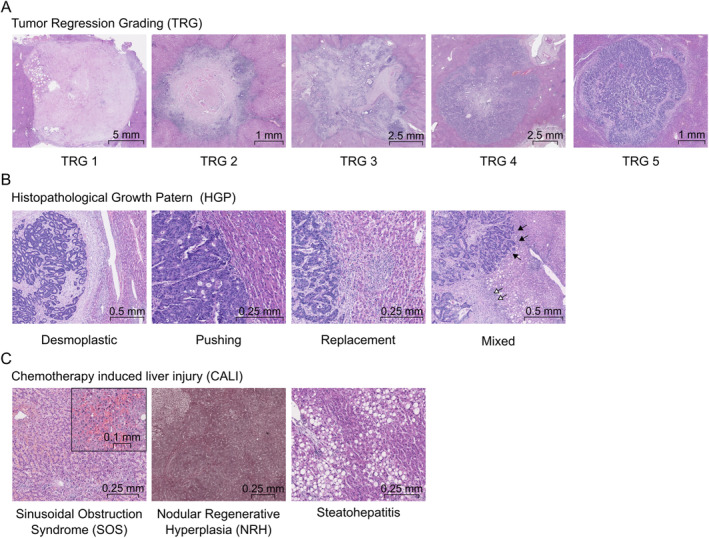
Keywords: Immunoscore; chemotherapy related liver injury; colorectal cancer; colorectal liver metastases; histopathological growth pattern; pathological score; steatohepatitis; tumor microenvironment; tumor regression grading.
© 2020 The Authors. The Journal of Pathology: Clinical Research published by The Pathological Society of Great Britain and Ireland and John Wiley & Sons Ltd.
Figures
Similar articles
-
Immunity to live: an immunopathoscore using the consensus Immunoscore to best define the risk of recurrence and death in stage IV metastatic patients.Oncoimmunology. 2020 Oct 13;9(1):1826133. doi: 10.1080/2162402X.2020.1826133. Oncoimmunology. 2020. PMID: 33110705 Free PMC article. Review.
-
Comprehensive Intrametastatic Immune Quantification and Major Impact of Immunoscore on Survival.J Natl Cancer Inst. 2018 Jan 1;110(1). doi: 10.1093/jnci/djx123. J Natl Cancer Inst. 2018. PMID: 28922789
-
The Immunoscore system predicts prognosis after liver metastasectomy in colorectal cancer liver metastases.Cancer Immunol Immunother. 2018 Mar;67(3):435-444. doi: 10.1007/s00262-017-2094-8. Epub 2017 Dec 4. Cancer Immunol Immunother. 2018. PMID: 29204700 Free PMC article.
-
BRAF mutation is a prognostic biomarker for colorectal liver metastasectomy.J Surg Oncol. 2012 Aug 1;106(2):123-9. doi: 10.1002/jso.23063. Epub 2012 Feb 13. J Surg Oncol. 2012. PMID: 22331825
-
The role of the pathologist and clinical implications in colorectal liver metastasis.Acta Gastroenterol Belg. 2018 Jul-Sep;81(3):419-426. Acta Gastroenterol Belg. 2018. PMID: 30350532 Review.
Cited by
-
Immunity to live: an immunopathoscore using the consensus Immunoscore to best define the risk of recurrence and death in stage IV metastatic patients.Oncoimmunology. 2020 Oct 13;9(1):1826133. doi: 10.1080/2162402X.2020.1826133. Oncoimmunology. 2020. PMID: 33110705 Free PMC article. Review.
-
Homogeneity in immune features between colorectal liver metastases better identifies patients with good prognosis compared to pathological response to preoperative chemotherapy.Oncoimmunology. 2023 Sep 14;12(1):2253642. doi: 10.1080/2162402X.2023.2253642. eCollection 2023. Oncoimmunology. 2023. PMID: 37720689 Free PMC article.
-
Histopathological Growth Pattern in Colorectal Liver Metastasis and The Tumor Immune Microenvironment.Cancers (Basel). 2022 Dec 28;15(1):181. doi: 10.3390/cancers15010181. Cancers (Basel). 2022. PMID: 36612177 Free PMC article. Review.
-
Prognostic Effect of CEA Cut-Off in Patients with Resectable Colorectal Liver Metastases: A Meta-Analysis and Meta-Regression.J Gastrointest Cancer. 2025 May 13;56(1):117. doi: 10.1007/s12029-025-01244-6. J Gastrointest Cancer. 2025. PMID: 40358861
-
Prognostic assessment of T-cells in primary colorectal cancer and paired synchronous or metachronous liver metastasis.Int J Cancer. 2025 Mar 15;156(6):1282-1292. doi: 10.1002/ijc.35252. Epub 2024 Nov 7. Int J Cancer. 2025. PMID: 39508720 Free PMC article.
References
-
- Van Cutsem E, Cervantes A, Adam R, et al ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann Oncol 2016; 27: 1386–1422. - PubMed
-
- Viganò L, Russolillo N, Ferrero A, et al Evolution of long‐term outcome of liver resection for colorectal metastases: analysis of actual 5‐year survival rates over two decades. Ann Surg Oncol 2012; 19: 2035–2044. - PubMed
-
- de Jong MC, Pulitano C, Ribero D, et al Rates and patterns of recurrence following curative intent surgery for colorectal liver metastasis: an international multi‐institutional analysis of 1669 patients. Ann Surg 2009; 250: 440–448. - PubMed
-
- Smith MD, McCall JL. Systematic review of tumour number and outcome after radical treatment of colorectal liver metastases. Br J Surg 2009; 96: 1101–1113. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
