

Subclinical cardiac dysfunction in obesity patients is linked to autonomic dysfunction: findings from the CARDIOBESE study
- PMID: 32902195
- PMCID: PMC7754761
- DOI: 10.1002/ehf2.12942
Subclinical cardiac dysfunction in obesity patients is linked to autonomic dysfunction: findings from the CARDIOBESE study
Abstract
Aims: Obesity doubles the lifetime risk of developing heart failure. Current knowledge on the role of obesity in causing cardiac dysfunction is insufficient for optimal risk stratification. The aim of this study was first to estimate the prevalence of subclinical cardiac dysfunction in obesity patients and second to investigate the underlying pathophysiology.
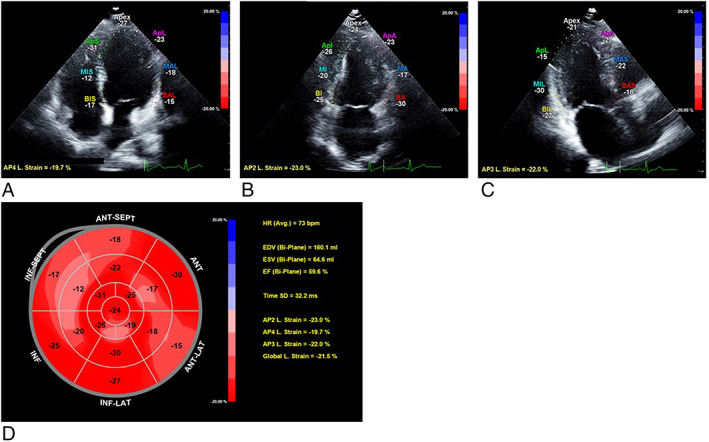
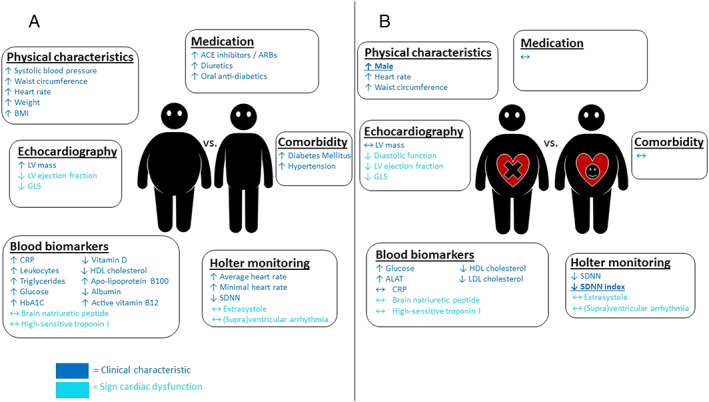
Methods and results: The CARDIOBESE study is a cross-sectional multicentre study of 100 obesity patients [body mass index (BMI) ≥ 35 kg/m2 ] without known cardiovascular disease and 50 age-matched and gender-matched non-obese controls (BMI ≤ 30 kg/m2 ). Echocardiography was performed, blood samples were collected, and a Holter monitor was affixed. Fifty-nine obesity patients [48 (42-50) years, 70% female] showed subclinical cardiac dysfunction: 57 patients had decreased global longitudinal strain (GLS), and two patients with normal GLS had either diastolic dysfunction or increased brain natriuretic peptide (BNP). Only one non-obese control had diastolic dysfunction, and none had another sign of cardiac dysfunction. Multivariable logistic analysis identified male gender and standard deviation of all NN intervals (SDNN) index, which is a measure of autonomic dysfunction, as independent significant risk factors for subclinical cardiac dysfunction in obesity patients.
Conclusions: There was a high prevalence (61%) of subclinical cardiac dysfunction in obesity patients without known cardiovascular disease, which appeared to be best identified by GLS. Subclinical cardiac dysfunction in obesity was linked to autonomic dysfunction and male gender, and not to the presence of traditional cardiac risk factors, increased C-reactive protein, increased BNP, increased high-sensitivity troponin I, or increased left ventricular mass.
Keywords: Cardiac dysfunction; Global longitudinal strain; Heart rate variability; Obesity/obese; Speckle-tracking echocardiography.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Afshin A, Reitsma MB, Murray CJL. Health effects of overweight and obesity in 195 countries. N Engl J Med 2017; 377: 1496–1497. - PubMed
-
- Global BMIMC , Di Angelantonio E, Bhupathiraju SN, Wormser D, Gao P, Kaptoge S, de Gonzalez AB, Cairns BJ, Huxley R, Jackson CL, Joshy G, Lewington S. Body‐mass index and all‐cause mortality: individual‐participant‐data meta‐analysis of 239 prospective studies in four continents. Lancet 2016; 388: 776–786. - PMC - PubMed
-
- Packer M. The conundrum of patients with obesity, exercise intolerance, elevated ventricular filling pressures and a measured ejection fraction in the normal range. Eur J Heart Fail 2019; 21: 156–162. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
