

Angular Location of Retinal Nerve Fiber Layer Defect: Association With Myopia and Open-Angle Glaucoma
- PMID: 32902578
- PMCID: PMC7488617
- DOI: 10.1167/iovs.61.11.13
Angular Location of Retinal Nerve Fiber Layer Defect: Association With Myopia and Open-Angle Glaucoma
Abstract
Purpose: To compare retinal nerve fiber layer (RNFL) defects' angle measurements determined from the center of the optic disc and Bruch's membrane opening (BMO), as a function of myopia and open-angle glaucoma (OAG) subtypes.
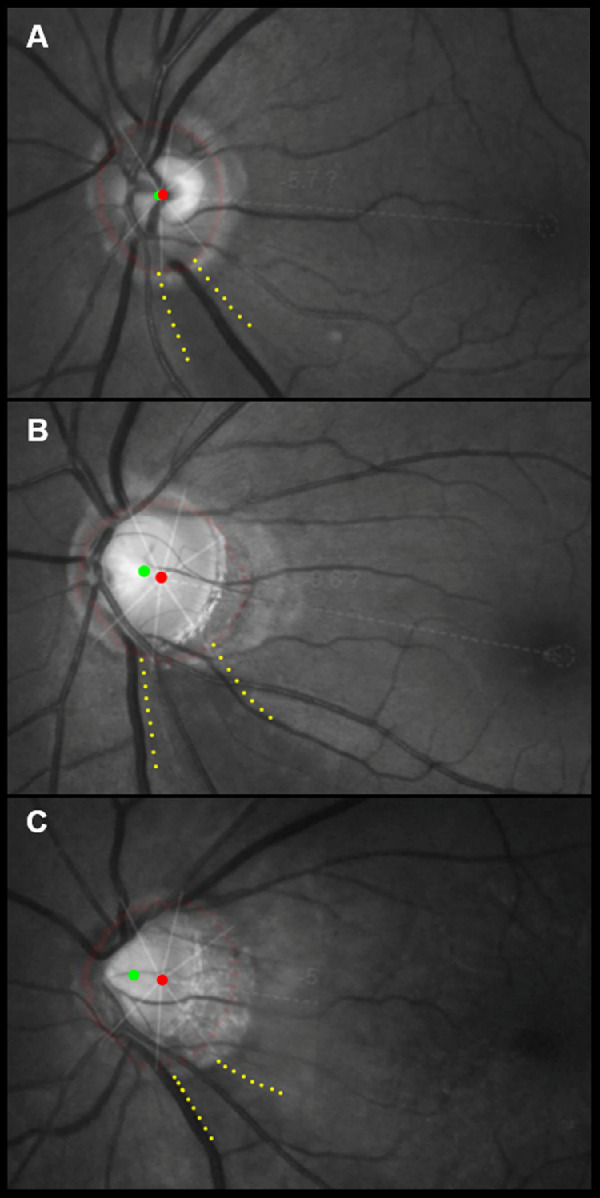
Methods: In total, 118 patients with OAG were grouped by axial length (AL; high myopia, AL >26 mm; mild to moderate myopia, 24 ≤ AL ≤26 mm; nonmyopia, AL <24 mm) and OAG subtype (normal-tension glaucoma [NTG], high-tension glaucoma [HTG]). The disc and BMO centers were determined by a merged image of red-free fundus photography and spectral-domain optical coherence tomography. The angular location of the RNFL defect close to the fovea (angle α) was measured from the disc center and BMO center, respectively (angle αdisc and angle αBMO). The difference between angle αdisc and αBMO (Δα), as well as the RNFL defect width (angle γ), was evaluated.
Results: Angle αdisc was smaller in myopic eyes and correlated significantly with AL (P = 0.001), whereas it did not differ among OAG subgroups. Angle αBMO and angle γ were not different in the myopic and OAG subgroups. The Δ α was larger for eyes with higher degree of myopia and had significant correlation with AL (P < 0.001) and was larger in NTG eyes than in HTG eyes (P = 0.023).
Conclusions: The angular location of the RNFL defect measured from the disc center, but not from the BMO center, was closer to the fovea for glaucomatous eyes with higher values of AL. The present study may facilitate understanding of the characteristic locational pattern of the RNFL defect in myopic glaucomatous eyes.
Conflict of interest statement
Disclosure:
Figures



Similar articles
-
Position of Central Retinal Vascular Trunk and Preferential Location of Glaucomatous Damage in Myopic Normal-Tension Glaucoma.Ophthalmol Glaucoma. 2018 Jul-Aug;1(1):32-43. doi: 10.1016/j.ogla.2018.05.003. Epub 2018 Jun 29. Ophthalmol Glaucoma. 2018. PMID: 32672631
-
Differences in Retinal Nerve Fiber Layer Thickness as Assessed on the Disc Center and Bruch's Membrane Opening Center in Myopic Eyes.Ophthalmol Glaucoma. 2019 May-Jun;2(3):145-155. doi: 10.1016/j.ogla.2019.02.008. Epub 2019 Mar 2. Ophthalmol Glaucoma. 2019. PMID: 32672582
-
Diagnostic Accuracy of Optical Coherence Tomography and Scanning Laser Tomography for Identifying Glaucoma in Myopic Eyes.Ophthalmology. 2016 Jun;123(6):1181-9. doi: 10.1016/j.ophtha.2016.01.052. Epub 2016 Mar 15. Ophthalmology. 2016. PMID: 26992843
-
Evaluating glaucoma in myopic eyes: Challenges and opportunities.Surv Ophthalmol. 2025 May-Jun;70(3):563-582. doi: 10.1016/j.survophthal.2024.12.003. Epub 2024 Dec 17. Surv Ophthalmol. 2025. PMID: 39701308 Review.
-
Implications of myopia in diagnosis and screening of open angle glaucoma.Curr Opin Ophthalmol. 2025 Mar 1;36(2):107-114. doi: 10.1097/ICU.0000000000001116. Epub 2024 Dec 23. Curr Opin Ophthalmol. 2025. PMID: 39705201 Review.
Cited by
-
Optic nerve head factors associated with initial central visual field defect in primary open-angle glaucoma.Sci Rep. 2024 Apr 5;14(1):8000. doi: 10.1038/s41598-024-58749-6. Sci Rep. 2024. PMID: 38580736 Free PMC article.
-
Offset of openings in optic nerve head canal at level of Bruch's membrane, anterior sclera, and lamina cribrosa.Sci Rep. 2021 Nov 17;11(1):22435. doi: 10.1038/s41598-021-01184-8. Sci Rep. 2021. PMID: 34789748 Free PMC article.
-
Forecasting Risk of Future Rapid Glaucoma Worsening Using Early Visual Field, OCT, and Clinical Data.Ophthalmol Glaucoma. 2023 Sep-Oct;6(5):466-473. doi: 10.1016/j.ogla.2023.03.005. Epub 2023 Mar 20. Ophthalmol Glaucoma. 2023. PMID: 36944385 Free PMC article.
-
Update on the Utility of Optical Coherence Tomography in the Analysis of the Optic Nerve Head in Highly Myopic Eyes with and without Glaucoma.J Clin Med. 2023 Mar 29;12(7):2592. doi: 10.3390/jcm12072592. J Clin Med. 2023. PMID: 37048675 Free PMC article. Review.
References
-
- Quigley HA, Addicks EM. Regional differences in the structure of the lamina cribrosa and their relation to glaucomatous optic nerve damage. Arch Ophthalmol. 1981; 99: 137–143. - PubMed
-
- Kanamori A, Nakamura M, Tomioka M, Kawaka Y, Yamada Y, Negi A. Structure-function relationship among three types of spectral-domain optical coherent tomography instruments in measuring parapapillary retinal nerve fibre layer thickness. Acta Ophthalmol. 2013; 91: e196–202. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
