

Association of Immunotherapy With Survival Among Patients With Brain Metastases Whose Cancer Was Managed With Definitive Surgery of the Primary Tumor
- PMID: 32902650
- PMCID: PMC7489857
- DOI: 10.1001/jamanetworkopen.2020.15444
Association of Immunotherapy With Survival Among Patients With Brain Metastases Whose Cancer Was Managed With Definitive Surgery of the Primary Tumor
Abstract
Importance: Immunotherapy has shown significant control of intracranial metastases in patients with melanoma. However, the association of immunotherapy combined with other cancer treatments and overall survival (OS) of patients with brain metastases, regardless of primary tumor site, is unknown.
Objective: To explore the association of immunotherapy with OS in patients with cancer and brain metastases who received definitive surgery of the primary site.
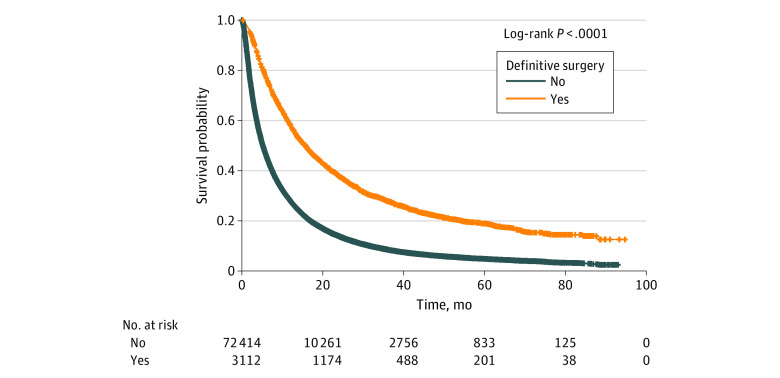
Design, setting, and participants: This comparative effectiveness study included 3112 adult patients in the National Cancer Database from 2010 to 2016 with non-small cell lung cancer, breast cancer, melanoma, colorectal cancer, or kidney cancer and brain metastases at the time of diagnosis and who received definitive surgery of the primary site. Data analysis was conducted from March to April 2020.
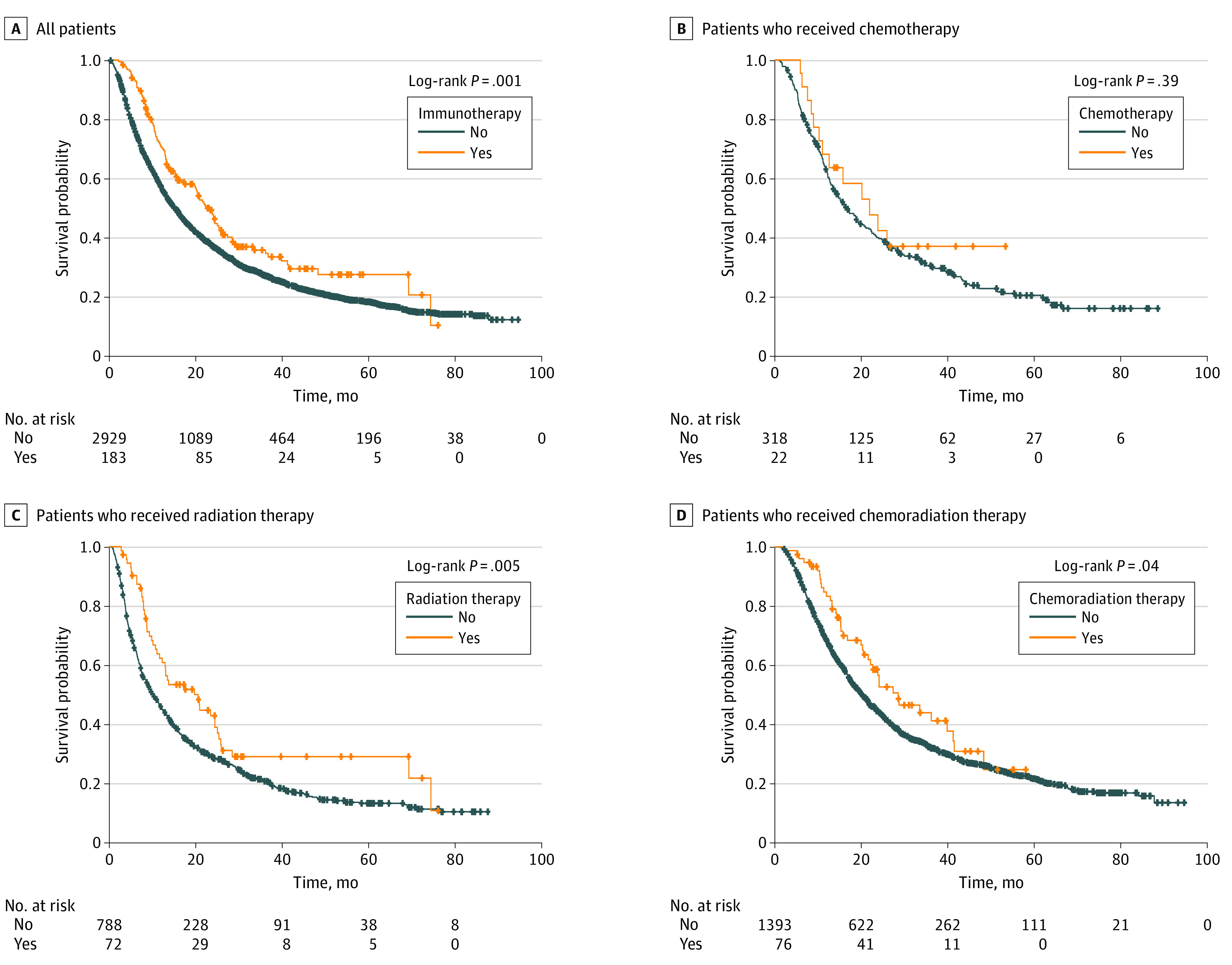
Exposures: Treatment groups were stratified as follows: (1) any treatment with or without immunotherapy, (2) chemotherapy with or without immunotherapy, (3) radiotherapy (RT) with or without immunotherapy, and (4) chemoradiation with or without immunotherapy.
Main outcomes and measures: The association of immunotherapy with OS was assessed with Cox proportional hazards regression, adjusted for age at diagnosis, race, sex, place of living, income, education, treatment facility type, primary tumor type, and year of diagnosis.
Results: Of 3112 patients, 1436 (46.14%) were men, 2714 (87.72%) were White individuals, 257 (8.31%) were Black individuals, and 123 (3.98%) belonged to other racial and ethnic groups. The median (range) age at diagnosis was 61 (19-90) years. Overall, 183 (5.88%) received immunotherapy, 318 (10.22%) received chemotherapy alone, 788 (25.32%) received RT alone, and 1393 (44.76%) received chemoradiation alone; 22 (6.47%) received chemotherapy plus immunotherapy, 72 (8.37%) received RT plus immunotherapy, and 76 (5.17%) received chemoradiation plus immunotherapy. In the multivariable analysis, patients who received immunotherapy had significantly improved OS compared with no immunotherapy (hazard ratio, 0.62; 95% CI, 0.51-0.76; P < .001). Treatment with RT plus immunotherapy was associated with significantly improved OS compared with RT alone (hazard ratio, 0.59; 95% CI, 0.42-0.84; P = .003). Chemotherapy plus immunotherapy or chemoradiation plus immunotherapy were not associated with improved OS in the multivariable analysis.
Conclusions and relevance: In this study, the addition of immunotherapy to RT was associated with improved OS compared with radiotherapy alone in patients with brain metastases who received definitive surgery of the primary tumor site.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
