

Incidence of childhood renal tumours: An international population-based study
- PMID: 32902866
- PMCID: PMC7689773
- DOI: 10.1002/ijc.33147
Incidence of childhood renal tumours: An international population-based study
Abstract
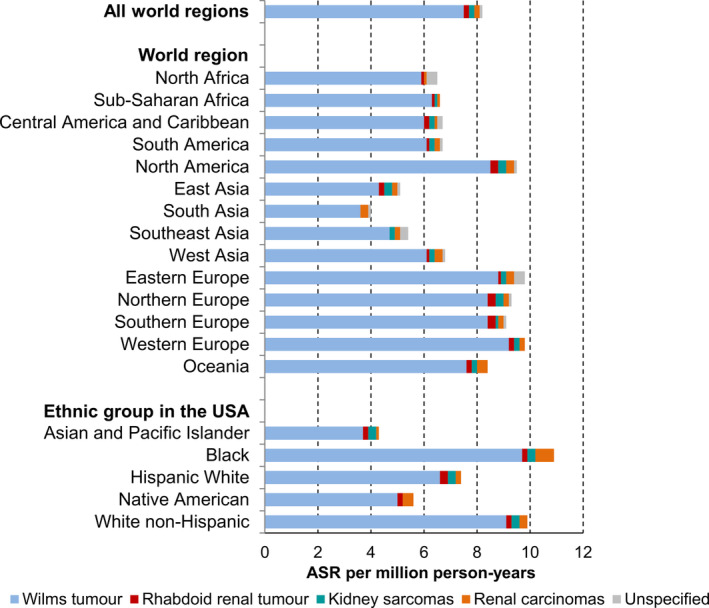
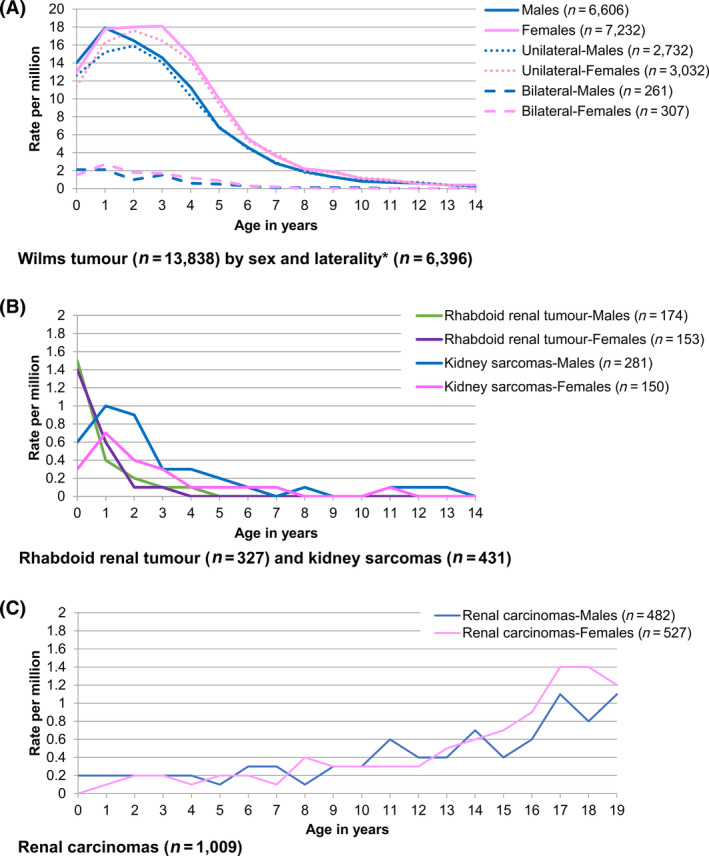
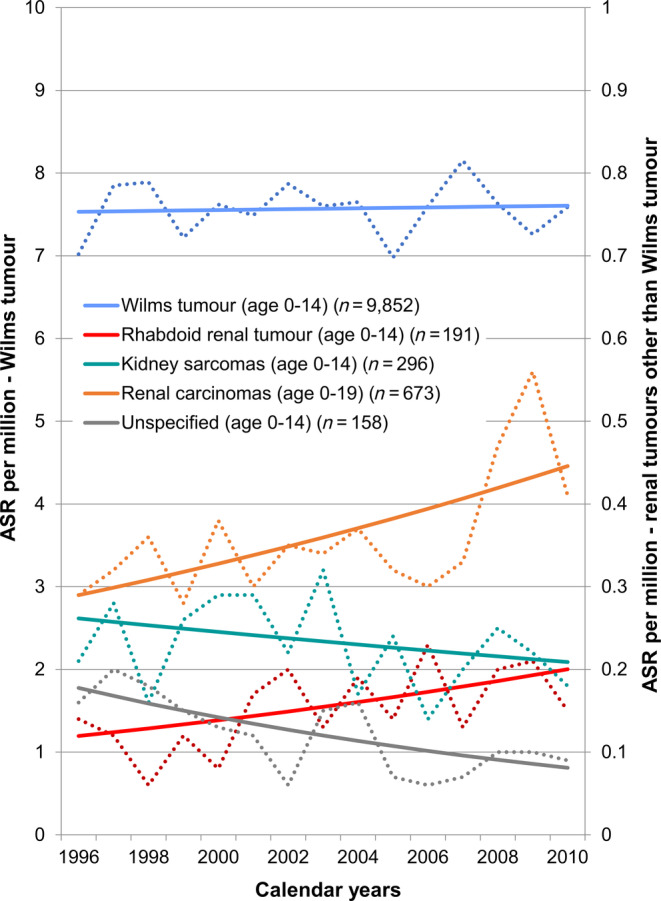
Malignant renal tumours represent 5% of childhood cancers and include types with likely different aetiology: Wilms tumour (WT), rhabdoid renal tumour, kidney sarcomas and renal carcinomas. WT is the most common renal tumour in children, previously shown to vary internationally and with ethnicity. Using the comprehensive database of the International Incidence of Childhood Cancer study (IICC), we analysed global variations and time trends in incidence of renal tumour types in children (age 0-14 years) and adolescents (age 15-19 years). The results were presented by 14 world regions, and five ethnic groups in the US. We included 15 320 renal tumours in children and 800 in adolescents reported to the 163 contributing registries during 2001-2010. In children, age-standardised incidence rate (ASR) of renal tumours was 8.3 per million (95% confidence interval, CI = 8.1, 8.4); it was the highest in North America and Europe (9-10 per million) and the lowest in most Asian regions (4-5 per million). In the US, Blacks had the highest ASR (10.9 per million, 95% CI = 10.2, 11.6) and Asian and Pacific Islanders the lowest (4.4 per million, 95% CI = 3.6, 5.1). In adolescents, age-specific incidence rate of renal tumours was 1.4 per million (95% CI = 1.3, 1.5). WT accounted for over 90% of all renal tumours in each age from 1 to 7 years and the proportion of renal carcinomas increased gradually with age. From 1996 to 2010, incidence remained mostly stable for WT (average annual percent change, AAPC = 0.1) and increased for renal carcinomas in children (AAPC = 3.7) and adolescents (AAPC = 3.2). Our findings warrant further monitoring.
Keywords: Wilms tumour; cancer epidemiology; childhood renal tumour; paediatric kidney cancer; population-based cancer registry study.
© 2020 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of Union for International Cancer Control.
Conflict of interest statement
All authors declare to have no conflict of interest.
Figures
References
-
- Pastore G, Znaor A, Spreafico F, Graf N, Pritchard‐Jones K, Steliarova‐Foucher E. Malignant renal tumours incidence and survival in European children (1978‐1997): report from the automated childhood cancer information system project. Eur J Cancer. 2006;42:2103‐2114. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
