

Screening Algorithms in Dense Breasts: AJR Expert Panel Narrative Review
- PMID: 32903054
- PMCID: PMC8101043
- DOI: 10.2214/AJR.20.24436
Screening Algorithms in Dense Breasts: AJR Expert Panel Narrative Review
Abstract
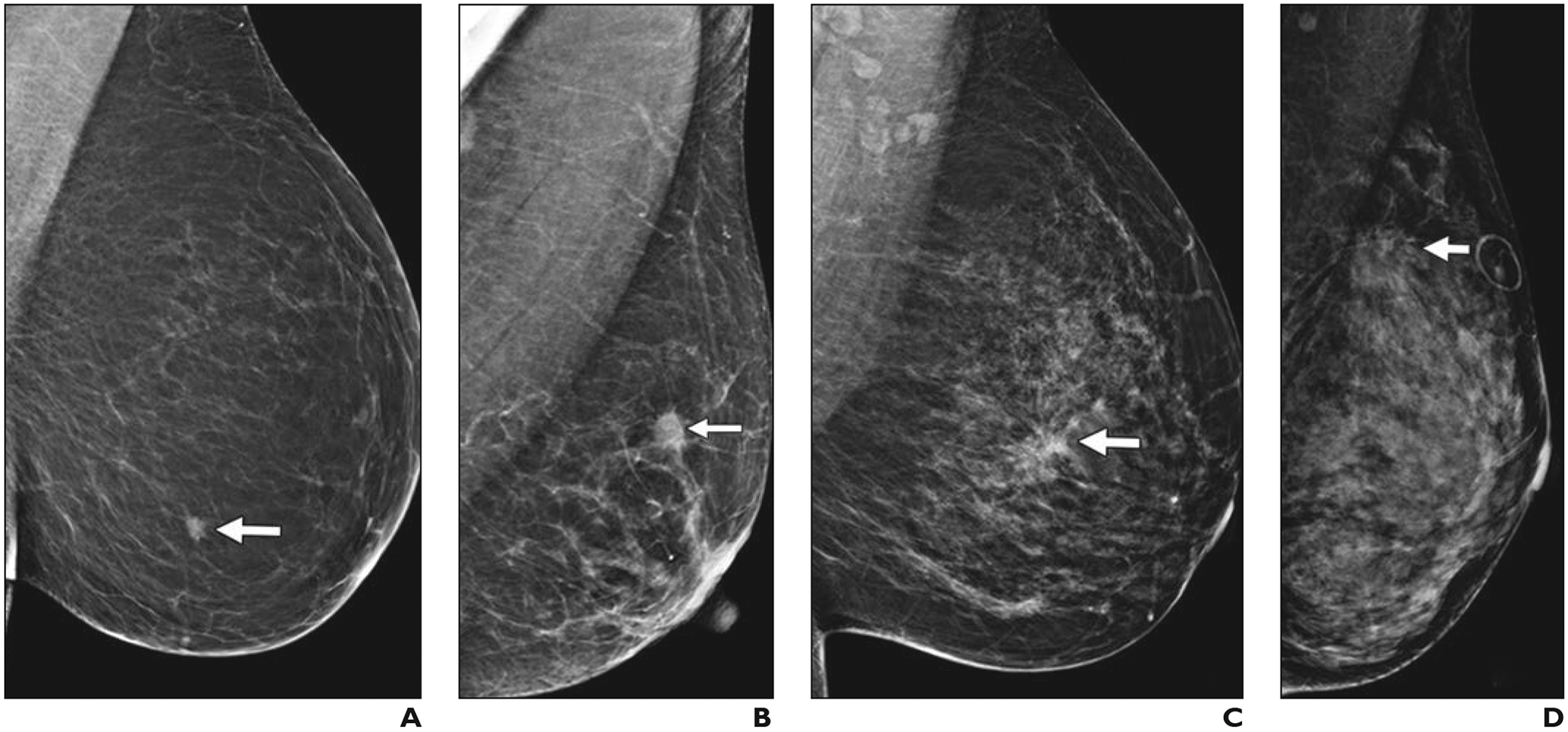
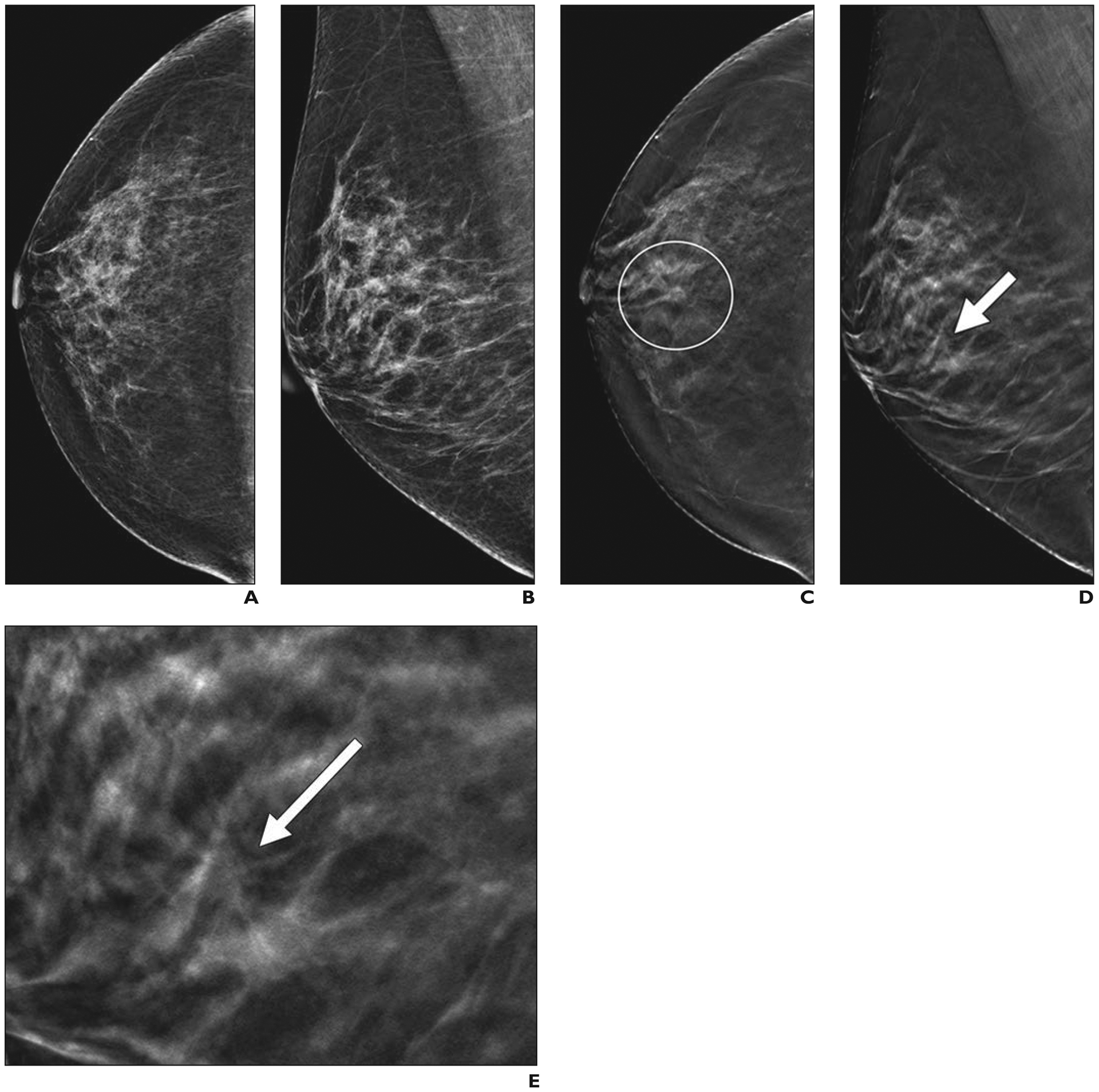
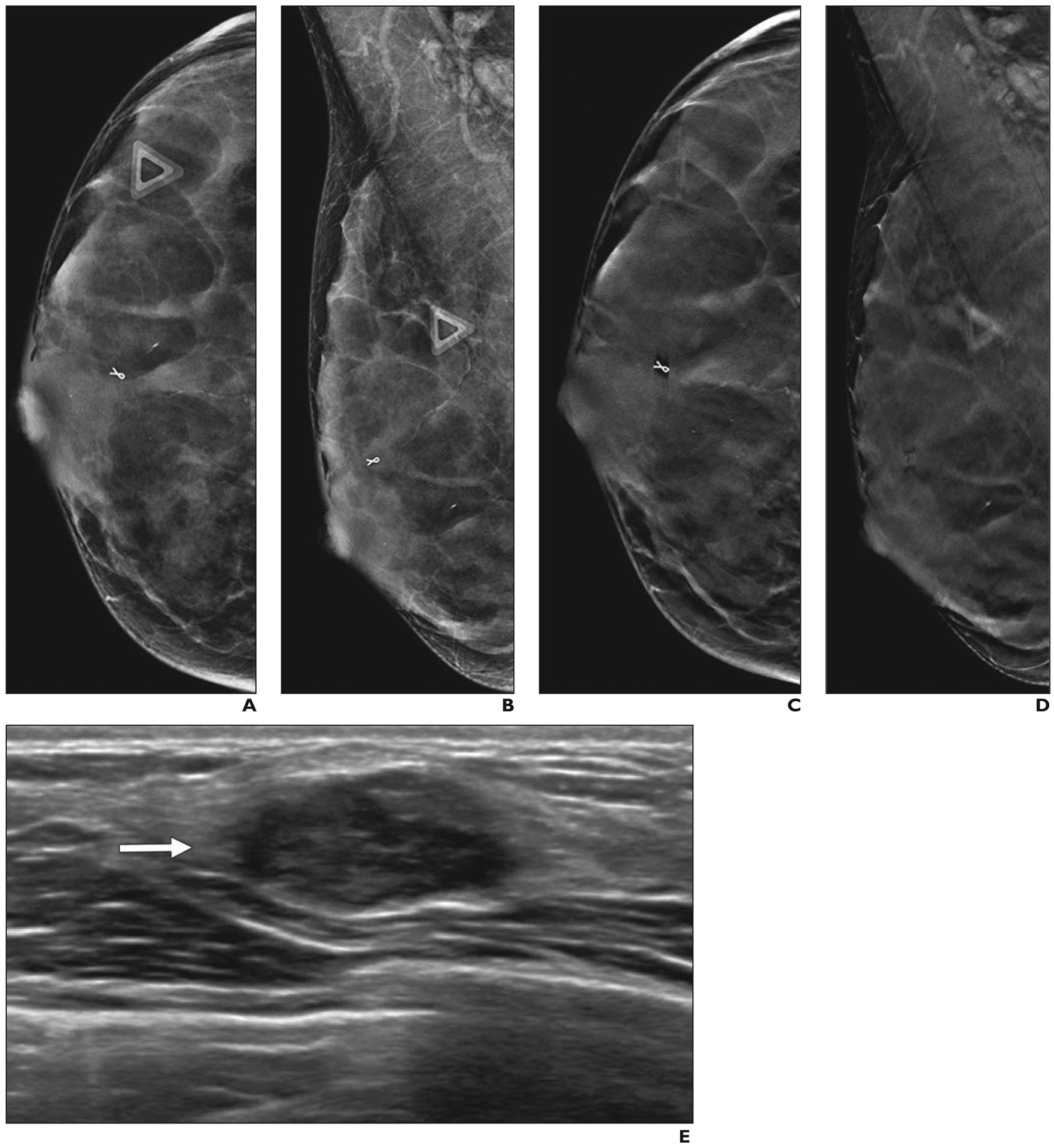
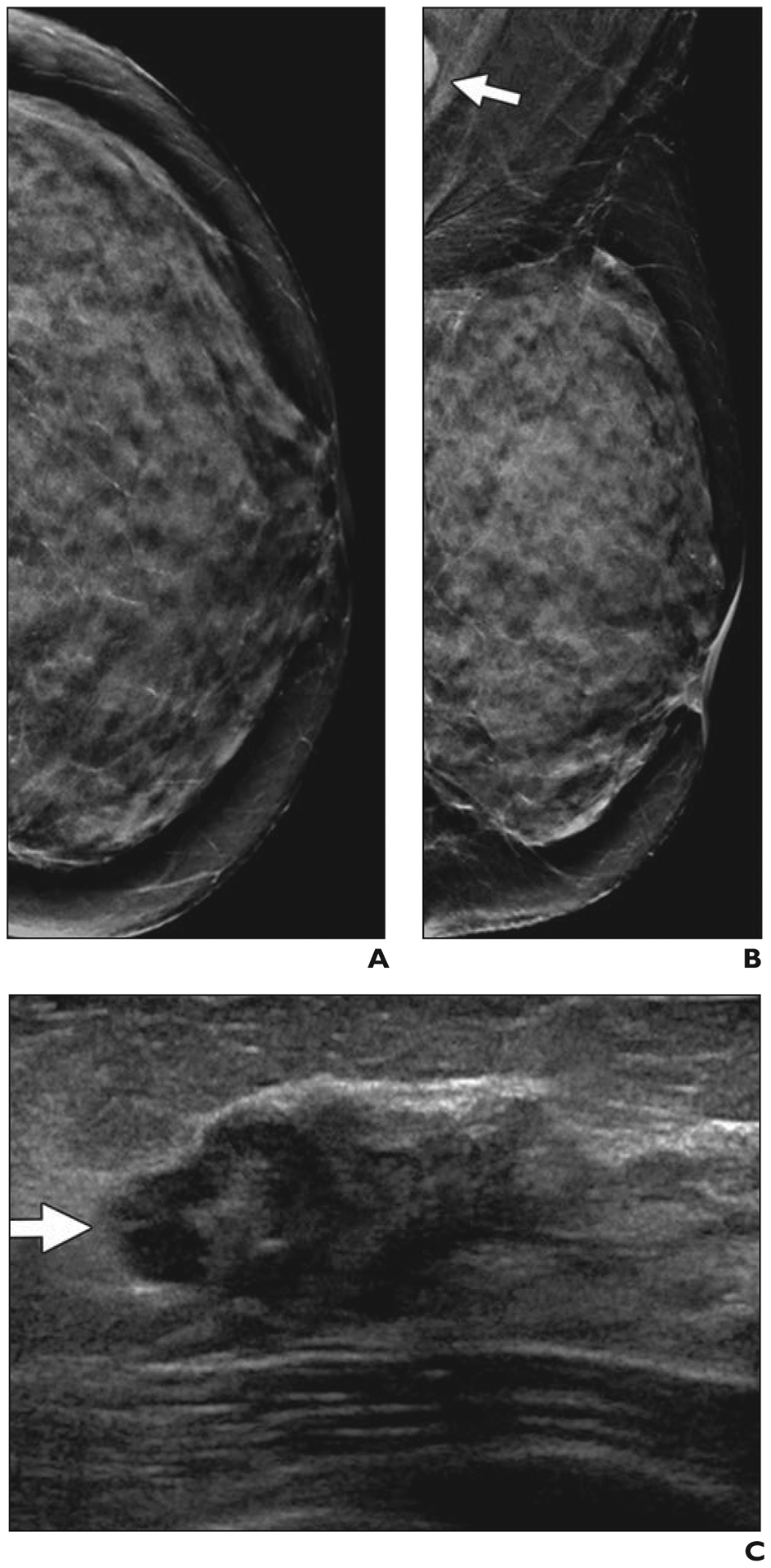
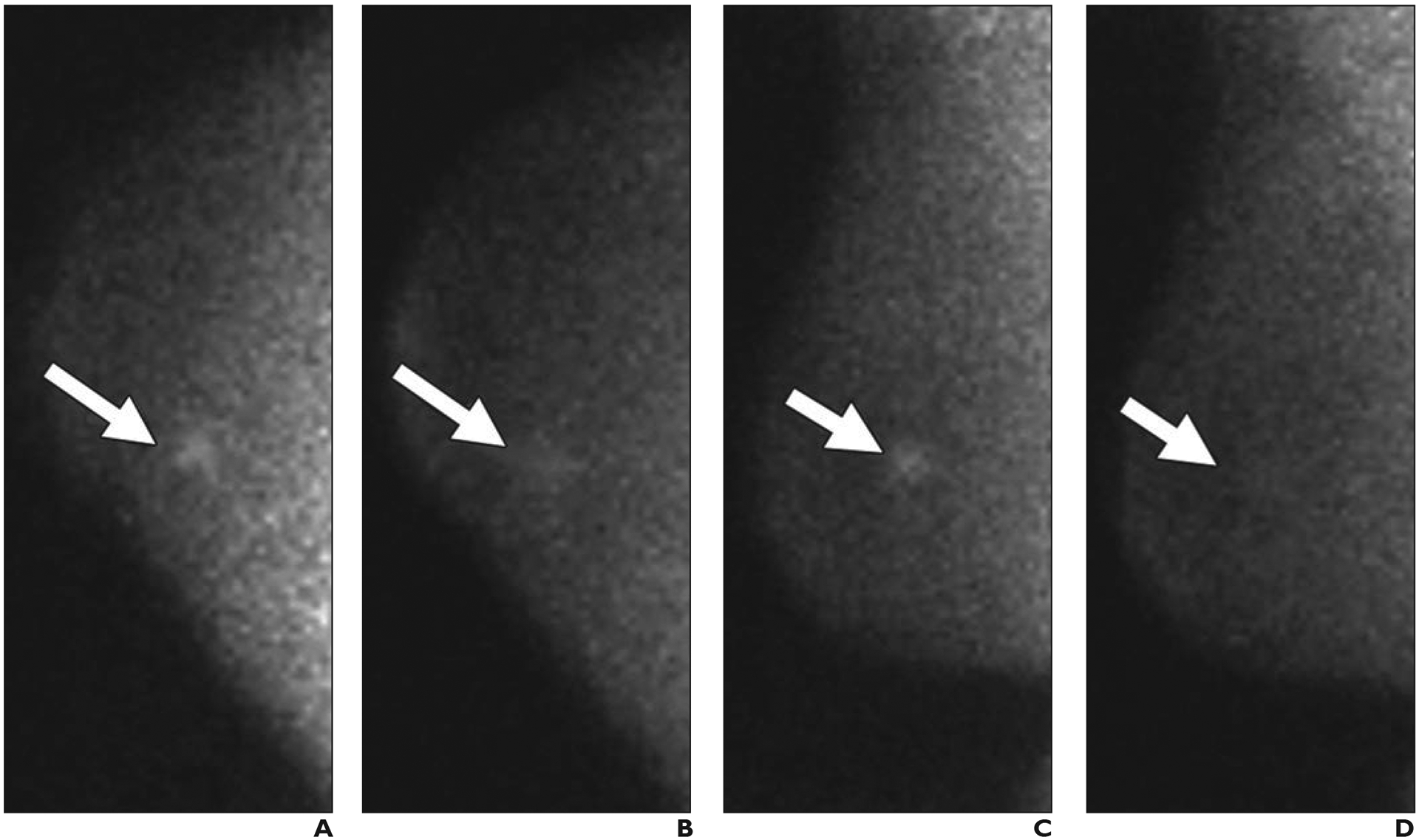
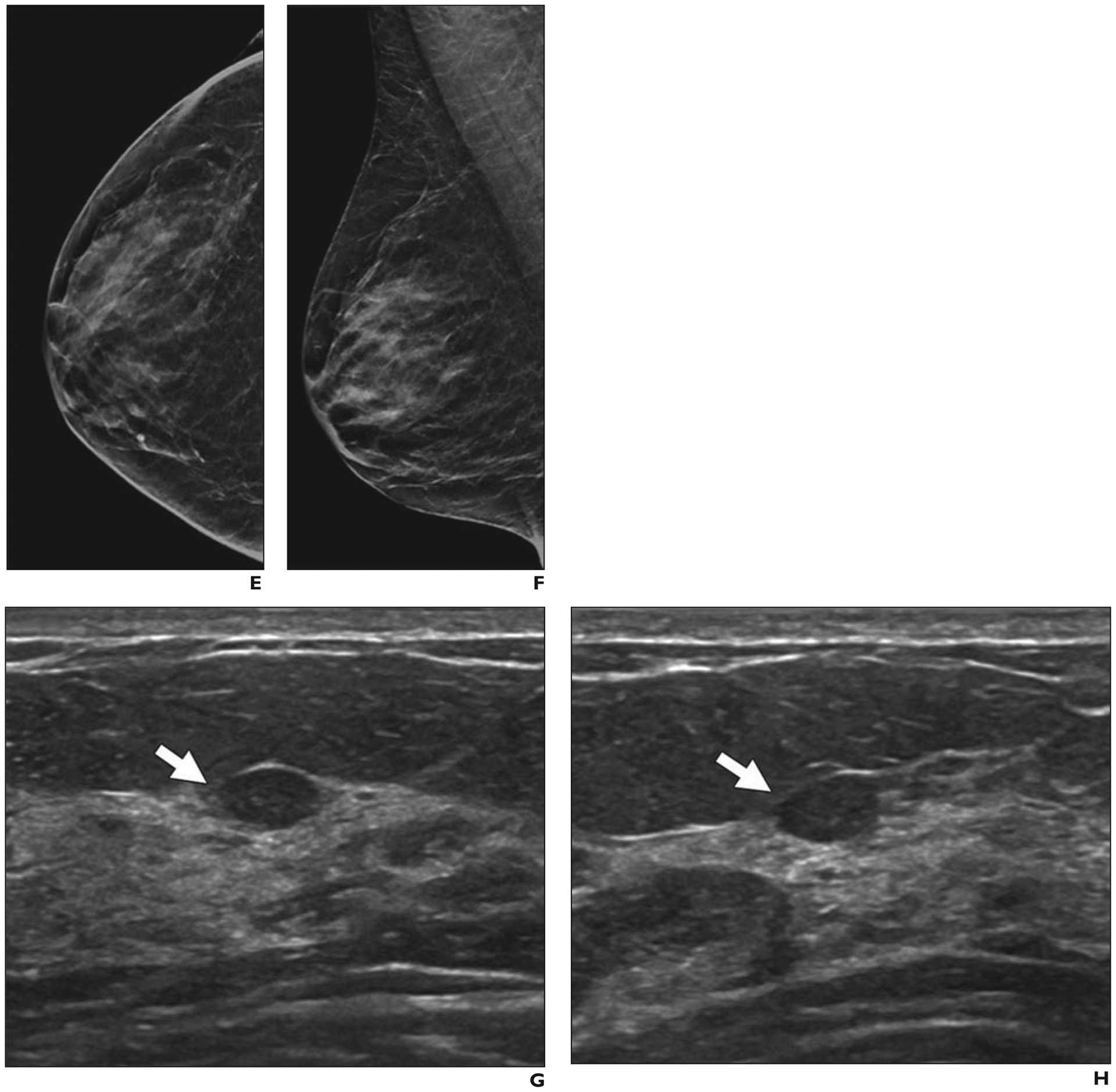
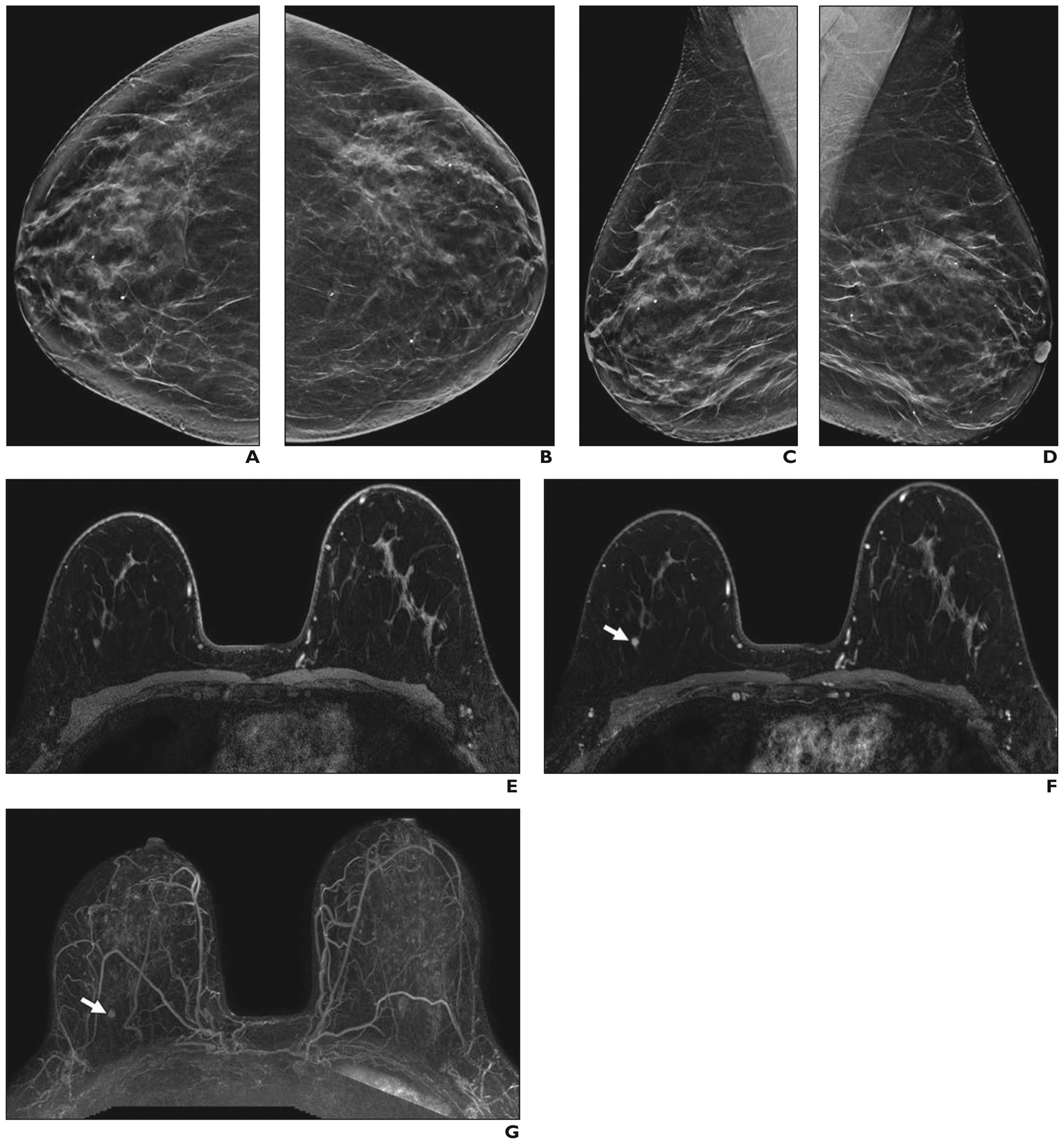
Screening mammography reduces breast cancer mortality; however, when used to examine women with dense breasts, its performance and resulting benefits are reduced. Increased breast density is an independent risk factor for breast cancer. Digital breast tomosynthesis (DBT), ultrasound (US), molecular breast imaging (MBI), MRI, and contrast-enhanced mammography (CEM) each have shown improved cancer detection in dense breasts when compared with 2D digital mammography (DM). DBT is the preferred mammographic technique for producing a simultaneous reduction in recalls (i.e., additional imaging). US further increases cancer detection after DM or DBT and reduces interval cancers (cancers detected in the interval between recommended screening examinations), but it also produces substantial additional false-positive findings. MBI improves cancer detection with an effective radiation dose that is approximately fourfold that of DM or DBT but is still within accepted limits. MRI provides the greatest increase in cancer detection and reduces interval cancers and late-stage disease; abbreviated techniques will reduce cost and improve availability. CEM appears to offer performance similar to that of MRI, but further validation is needed. Dense breast notification will soon be a national standard; therefore, understanding the performance of mammography and supplemental modalities is necessary to optimize screening for women with dense breasts.
Keywords: MRI; breast density; contrast-enhanced mammography; molecular breast imaging; tomosynthesis; ultrasound.
Figures
Comment in
-
Breast MRI for "the Masses".Eur Radiol. 2022 Jun;32(6):4034-4035. doi: 10.1007/s00330-022-08782-8. Epub 2022 Apr 14. Eur Radiol. 2022. PMID: 35420302 No abstract available.
References
-
- Coldman A, Phillips N, Wilson C, et al. Pan-Canadian study of mammography screening and mortality from breast cancer. J Natl Cancer Inst 2014; 106:dju261. - PubMed
-
- Tabár L, Vitak B, Chen TH, et al. Swedish two-county trial: impact of mammographic screening on breast cancer mortality during 3 decades. Radiology 2011; 260:658–663 - PubMed
-
- Monticciolo DL, Newell MS, Hendrick RE, et al. Breast cancer screening for average-risk women: recommendations from the ACR Commission on Breast Imaging. J Am Coll Radiol 2017; 14:1137–1143 - PubMed
-
- Siu AL US Preventive Services Task Force. Screening for breast cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2016; 164:279–296 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
