

A biomechanical test model for evaluating osseous and osteochondral tissue adhesives
- PMID: 32903290
- PMCID: PMC7422571
- DOI: 10.1186/s42490-019-0011-2
A biomechanical test model for evaluating osseous and osteochondral tissue adhesives
Abstract
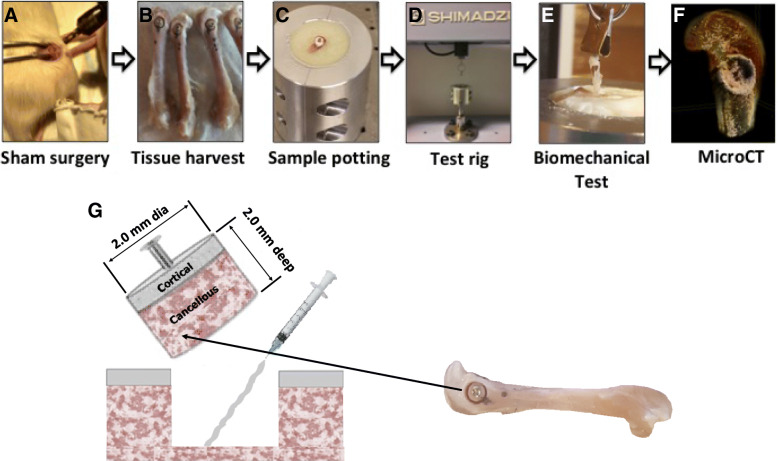
Background: Currently there are no standard models with which to evaluate the biomechanical performance of calcified tissue adhesives, in vivo. We present, herein, a pre-clinical murine distal femoral bone model for evaluating tissue adhesives intended for use in both osseous and osteochondral tissue reconstruction.
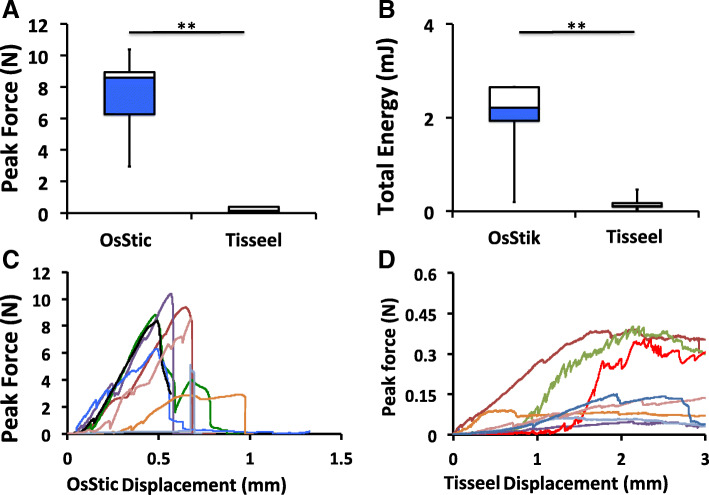
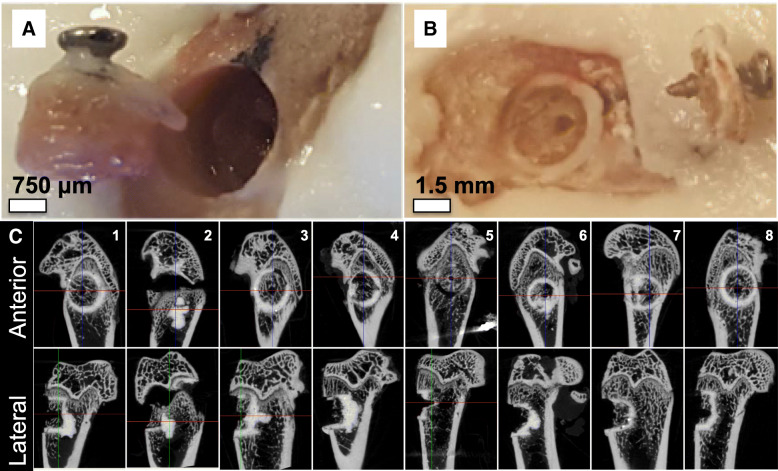
Results: Cylindrical cores (diameter (Ø) 2 mm (mm) × 2 mm depth), containing both cancellous and cortical bone, were fractured out from the distal femur and then reattached using one of two tissue adhesives. The adhesiveness of fibrin glue (Tisseeltm), and a novel, biocompatible, calcium phosphate-based tissue adhesive (OsStictm) were evaluated by pullout testing, in which glued cores were extracted and the peak force at failure recorded. The results show that Tisseel weakly bonded the metaphyseal bone cores, while OsStic produced > 30-fold higher mean peak forces at failure (7.64 Newtons (N) vs. 0.21 N). The failure modes were consistently disparate, with Tisseel failing gradually, while OsStic failed abruptly, as would be expected with a calcium-based material. Imaging of the bone/adhesive interface with microcomputed tomography revealed that, for OsStic, failure occurred more often within cancellous bone (75% of tested samples) rather than at the adhesive interface.
Conclusions: Despite the challenges associated with biomechanical testing in small rodent models the preclinical ex-vivo test model presented herein is both sensitive and accurate. It enabled differences in tissue adhesive strength to be quantified even for very small osseous fragments (<Ø4mm). Importantly, this model can easily be scaled to larger animals and adapted to fracture fragment fixation in human bone. The present model is also compatible with other long-term in vivo evaluation methods (i.e. in vivo imaging, histological analysis, etc.).
Keywords: Biomechanical model; Bone adhesive; Calcium phosphate cements; Fracture repair; Orthobiologics; Phosphoserine; Tissue adhesive.
© The Author(s) 2019.
Conflict of interest statement
Competing interestsThe following authors declare partial ownership in a company that owns all related intellectual property (GPBio LTD): Michael Pujari-Palmer (M.P.), Gerard Insley (G.I.), Philip Procter (P.P.), Håkan Engqvist (H.E.).
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources