

Patterns of lower limb muscular activity and joint moments during directional efforts using a static dynamometer
- PMID: 32903350
- PMCID: PMC7422517
- DOI: 10.1186/s42490-019-0035-7
Patterns of lower limb muscular activity and joint moments during directional efforts using a static dynamometer
Abstract
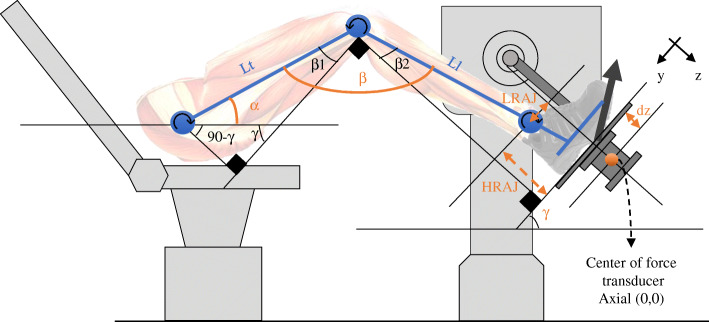
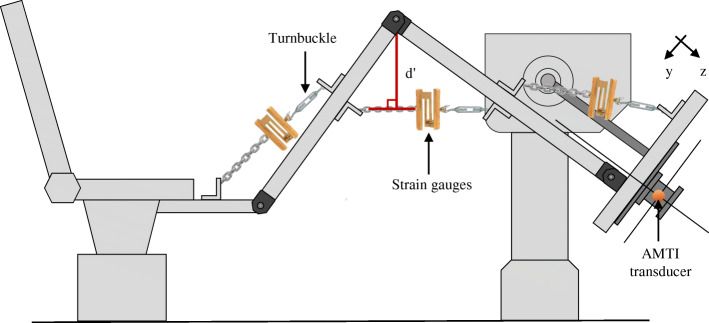
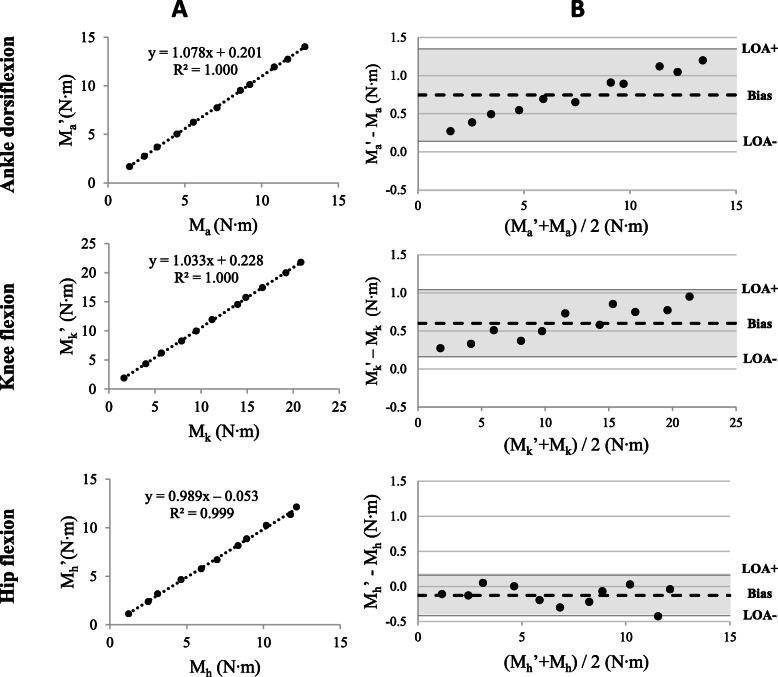
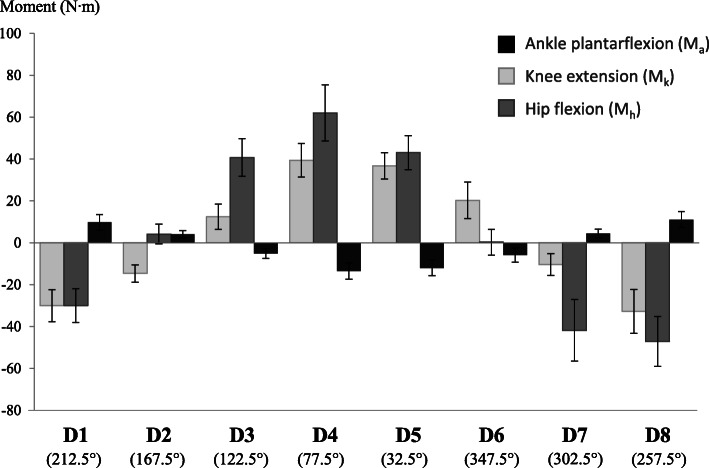
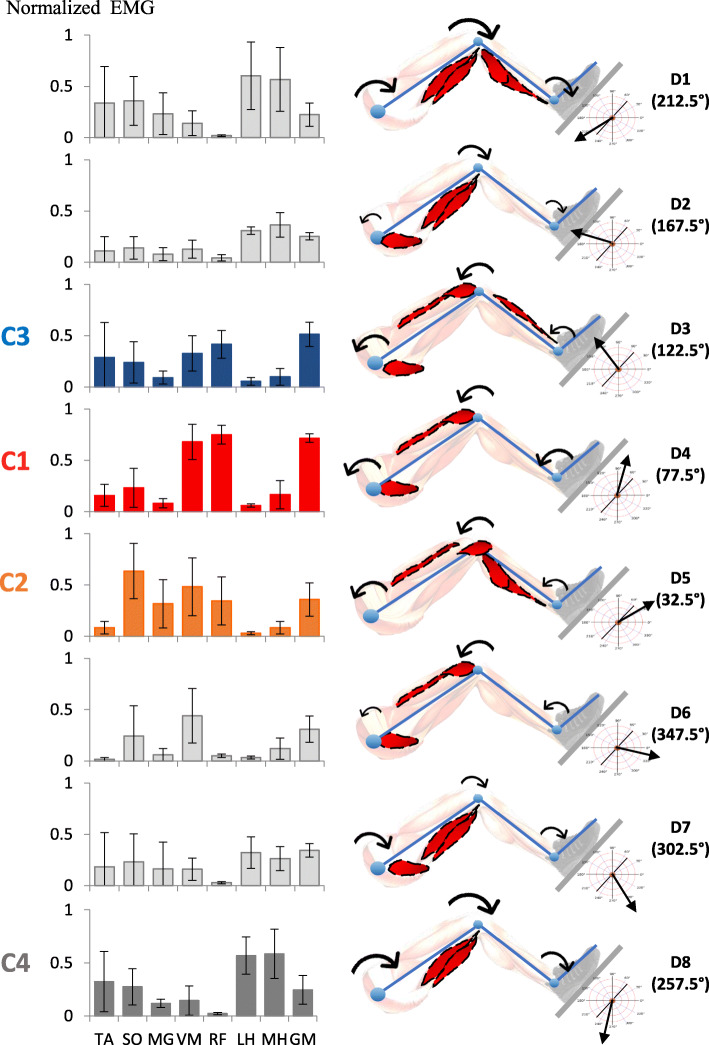
Background: Strength and coordination of lower muscle groups typically identified in healthy subjects are two prerequisites to performing functional activities. These physical qualities can be impaired following a neurological insult. A static dynamometer apparatus that measures lower limb joint moments during directional efforts at the foot was developed to recruit different patterns of muscular activity. The objectives of the present study were to 1) validate joint moments estimated by the apparatus, and 2) to characterize lower limb joint moments and muscular activity patterns of healthy subjects during progressive static efforts. Subjects were seated in a semi-reclined position with one foot attached to a force platform interfaced with a laboratory computer. Forces and moments exerted under the foot were computed using inverse dynamics, allowing for the estimation of lower limb joint moments.To achieve the study's first objective, joint moments were validated by comparing moments of various magnitudes of force applied by turnbuckles on an instrumented leg equipped with strain gauges with those estimated by the apparatus. Concurrent validity and agreement were assessed using Pearson correlation coefficients and Bland and Altman analysis, respectively. For the second objective, joint moments and muscular activity were characterized for five healthy subjects while exerting progressive effort in eight sagittal directions. Lower limb joint moments were estimated during directional efforts using inverse dynamics. Muscular activity of eight muscles of the lower limb was recorded using surface electrodes and further analyzed using normalized root mean square data.
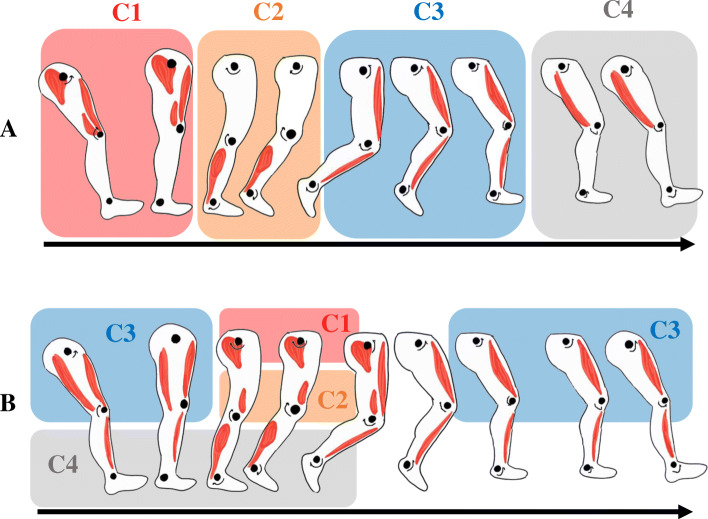
Results: The joint moments estimated with the instrumented leg were correlated (r > 0.999) with those measured by the dynamometer. Limits of agreement ranged between 8.5 and 19.2% of the average joint moment calculated by both devices. During progressive efforts on the apparatus, joint moments and patterns of muscular activity were specific to the direction of effort. Patterns of muscular activity in four directions were similar to activation patterns reported in the literature for specific portions of gait cycle.
Conclusion: This apparatus provides valid joint moments exerted at the lower limbs. It is suggested that this methodology be used to recruit muscular activity patterns impaired in neurological populations.
Keywords: (3–10) dynamometer; Electromyography; Gait; Lower limb; Muscle strength; Rehabilitation.
© The Author(s) 2020.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests related to the presented research.
Figures

References
LinkOut - more resources
Full Text Sources