

Transcatheter Tricuspid Valve Intervention: Coaptation Devices
- PMID: 32903754
- PMCID: PMC7438895
- DOI: 10.3389/fcvm.2020.00139
Transcatheter Tricuspid Valve Intervention: Coaptation Devices
Abstract
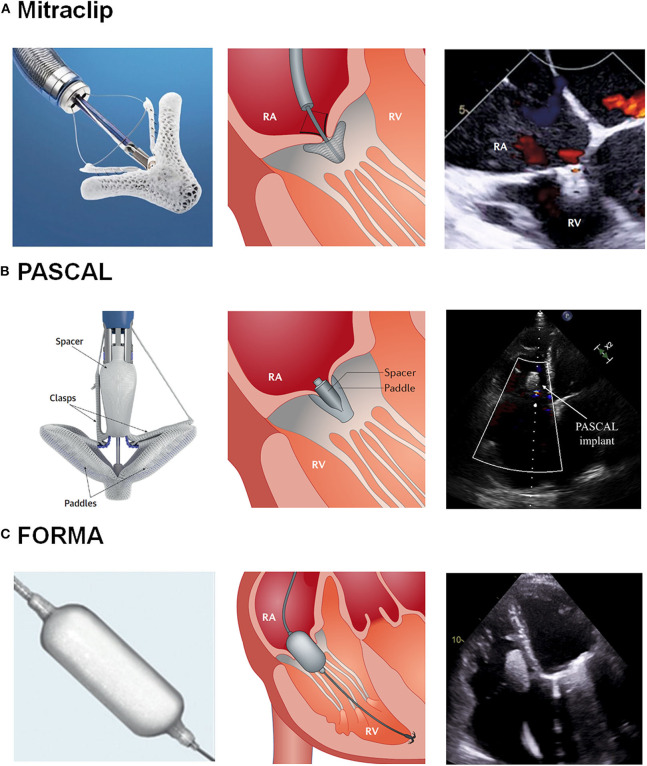
Transcatheter tricuspid valve intervention (TTVI) has recently emerged as an alternative for the treatment of severe tricuspid regurgitation (TR). Multiple percutaneous devices have been developed in the last decade with promising early results. Among them, the coaptation devices are designed to reduce TR severity by valve leaflet plication or occupying the regurgitant orifice with a spacer. To date, the MitraClip/TriClip devices (Abbott, Santa Clara, CA, USA), the PASCAL system (Edwards Lifesciencies, Irvine, CA, USA), and the FORMA device (Edwards Lifesciencies, Irvine, CA, USA) have been used as coaptation devices for treating severe TR. The present document aimed to review the clinical evidence on coaptation devices in the field of TTVI, describing its design characteristics, main procedural steps, and early and mid-term outcomes.
Keywords: FORMA; MitraClip device; PASCAL; transcatheter tricuspid intervention; tricuspid regurgitation (TR).
Copyright © 2020 Muntané-Carol, Alperi, Faroux, Bédard, Philippon and Rodés-Cabau.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources