

Clinical Outcome of Arthroscopic Partial Repair of Large to Massive Posterosuperior Rotator Cuff Tears: Medialization of the Attachment Site of the Rotator Cuff Tendon
- PMID: 32904088
- PMCID: PMC7449848
- DOI: 10.4055/cios19126
Clinical Outcome of Arthroscopic Partial Repair of Large to Massive Posterosuperior Rotator Cuff Tears: Medialization of the Attachment Site of the Rotator Cuff Tendon
Abstract
Backgroud: The goal of this study was to evaluate the clinical and radiological outcomes of arthroscopic partial repair with medialization of the attachment site of the rotator cuff tendon and to identify prognostic factors affecting rotator cuff healing in patients with irreparable large to massive posterosuperior rotator cuff tears.
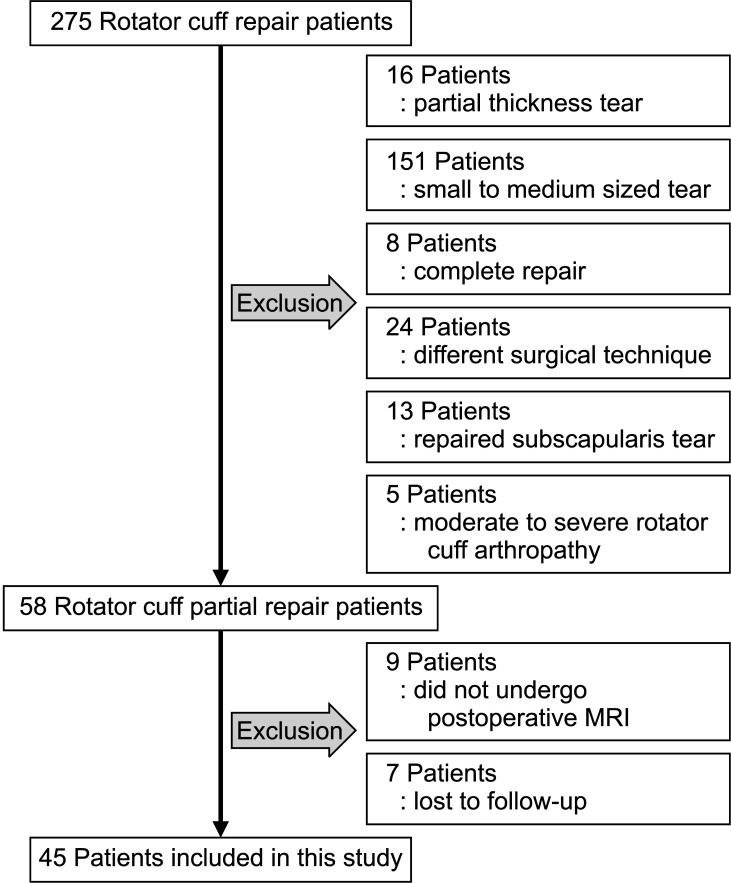
Methods: Between July 2012 and March 2016, 42 patients with irreparable large to massive posterosuperior rotator cuff tears underwent an arthroscopic partial repair with medialization of the attachment site of the rotator cuff tendon. All patients had a minimum of 2-year follow-up (mean, 35.4 ± 7.3 months). Clinical evaluation was performed using the visual analog scale, the University of California, Los Angeles shoulder rating scale, Constant score, and active range of motion. Radiological evaluation was performed using magnetic resonance imaging and simple radiography.
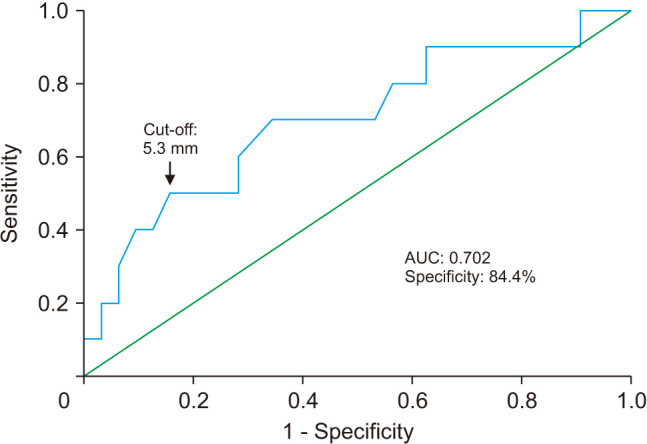
Results: Clinical outcomes at the final follow-up improved significantly compared with the preoperative values (all p < 0.001). The failure rate was 23.8% (10/42); however, clinical outcomes significantly improved regardless of cuff healing (all p < 0.001). The mean acromiohumeral distance was 6.5 ± 1.7 mm (range, 3.2-9.7 mm) before surgery and 6.3 ± 1.6 mm (range, 2.8-9.5 mm) at the final follow-up. Preoperative acromiohumeral distance was associated with failure of cuff healing in the univariate analysis (p = 0.043) and multivariate analysis (p = 0.048). A receiver operating characteristic curve was used to determine the predictive cutoff value for the smallest preoperative acromiohumeral distance for successful healing, which was calculated as 5.3 mm.
Conclusions: Despite healing failure, arthroscopic partial repair with medialization can be a possible treatment option for irreparable large to massive posterosuperior rotator cuff tears because of the improvement in clinical outcome. The shorter preoperative acromiohumeral distance was the single most important factor negatively affecting cuff healing, and the likelihood of success of healing might be improved if a repair is performed when the preoperative acromiohumeral distance is < 5.3 mm.
Keywords: Prognosis; Rotator cuff injuries; Shoulder.
Copyright © 2020 by The Korean Orthopaedic Association.
Conflict of interest statement
CONFLICT OF INTEREST: No potential conflict of interest relevant to this article was reported.
Figures

References
-
- McKee MD, Yoo DJ. The effect of surgery for rotator cuff disease on general health status: results of a prospective trial. J Bone Joint Surg Am. 2000;82(7):970–979. - PubMed
-
- Shin YK, Ryu KN, Park JS, Jin W, Park SY, Yoon YC. Predictive factors of retear in patients with repaired rotator cuff tear on shoulder MRI. AJR Am J Roentgenol. 2018;210(1):134–141. - PubMed
-
- Gerber C, Fuchs B, Hodler J. The results of repair of massive tears of the rotator cuff. J Bone Joint Surg Am. 2000;82(4):505–515. - PubMed
-
- Kim YK, Jung KH, Won JS, Cho SH. Medialized repair for retracted rotator cuff tears. J Shoulder Elbow Surg. 2017;26(8):1432–1440. - PubMed
-
- Burkhart SS, Nottage WM, Ogilvie-Harris DJ, Kohn HS, Pachelli A. Partial repair of irreparable rotator cuff tears. Arthroscopy. 1994;10(4):363–370. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
