

High practice variation in risk stratification, baseline oncological staging, and follow-up strategies for T1 colorectal cancers in the Netherlands
- PMID: 32904821
- PMCID: PMC7458727
- DOI: 10.1055/a-1192-3545
High practice variation in risk stratification, baseline oncological staging, and follow-up strategies for T1 colorectal cancers in the Netherlands
Abstract
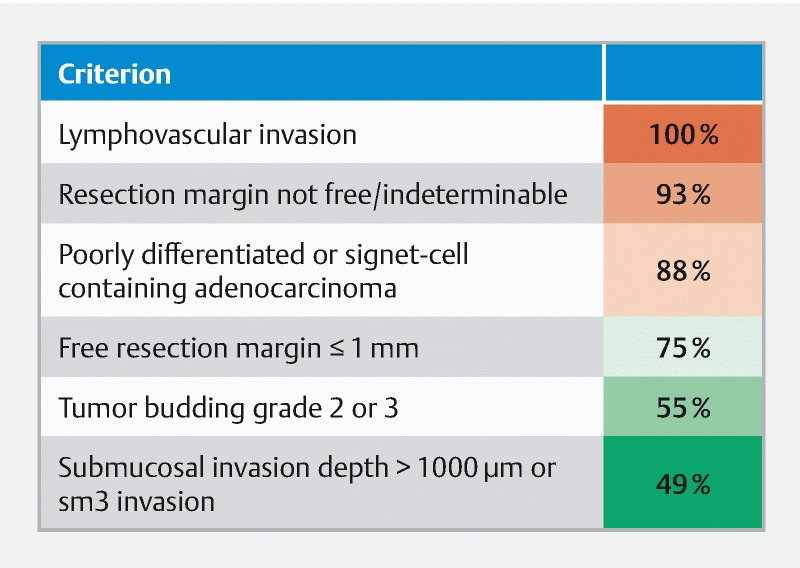
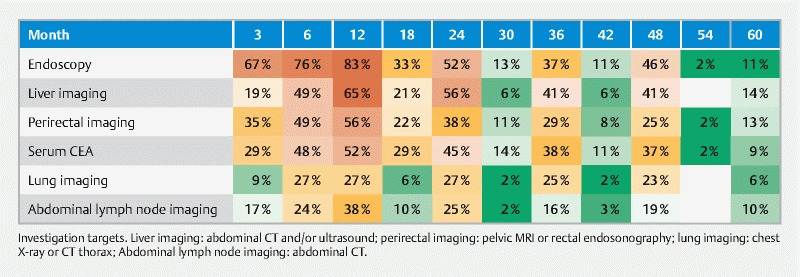
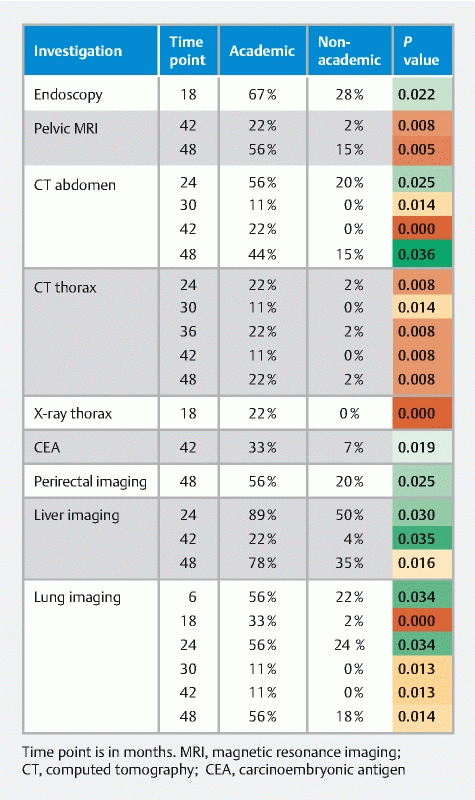
Background and study aims Based on pathology, locally resected T1 colorectal cancer (T1-CRC) can be classified as having low- or high-risk for irradicality and/or lymph node metastasis, the latter requiring adjuvant surgery. Reporting and application of pathological high-risk criteria is likely variable, with inherited variation regarding baseline oncological staging, treatment and surveillance. Methods We assessed practice variation using an online survey among gastroenterologists and surgeons participating in the Dutch T1-CRC Working Group. Results Of the 130 invited physicians, 53 % participated. Regarding high-risk T1-CRC criteria, lymphangio-invasion is used by 100 %, positive or indeterminable margins by 93 %, poor differentiation by 90 %, tumor-free margin ≤ 1 mm by 78 %, tumor budding by 57 % and submucosal invasion > 1000 µm by 47 %. Fifty-two percent of the respondents do not perform baseline staging in locally resected low-risk T1-CRC. In case of unoperated high-risk patients, we recorded 61 different surveillance strategies in 63 participants, using 19 different combinations of diagnostic tests. Endoscopy is used in all schedules. Mean follow-up time is 36 months for endoscopy, 26 months for rectal MRI and 30 months for abdominal CT (all varying 3-60 months). Conclusion We found variable use of pathological high-risk T1-CRC criteria, creating risk for misclassification as low-risk T1-CRC. This has serious implications, as most participants will not proceed to oncological staging in low-risk patients and adjuvant surgery nor radiological surveillance is considered. On the other hand, oncological surveillance in patients with a locally resected high-risk T1-CRC who do not wish adjuvant surgery is highly variable emphasizing the need for a uniform surveillance protocol.
Conflict of interest statement
Competing interests The authors declare that they have no conflict of interest.
Figures
Comment in
-
Considerable practice variation in use of pathological high-risk T1-CRC criteria: Why, and how to do better?Endosc Int Open. 2020 Oct;8(10):E1502-E1503. doi: 10.1055/a-1243-0129. Epub 2020 Oct 7. Endosc Int Open. 2020. PMID: 33043120 Free PMC article. No abstract available.
References
-
- Mengual-Ballester M, Pellicer-Franco E, Valero-Navarro G et al.Increased survival and decreased recurrence in colorectal cancer patients diagnosed in a screening programme. Cancer Epidemiol. 2016;43:70–75. - PubMed
-
- Backes Y, de Vos Tot Nederveen Cappel W H, van Bergeijk J et al.Risk for Incomplete Resection after Macroscopic Radical Endoscopic Resection of T1 Colorectal Cancer: A Multicenter Cohort Study. Am J Gastroenterol. 2017;112:785–796. - PubMed
-
- Ikematsu H, Yoda Y, Matsuda T et al.Long-term outcomes after resection for submucosal invasive colorectal cancers. Gastroenterology. 2013;144:551–559; quiz e514. - PubMed
-
- Yoda Y, Ikematsu H, Matsuda T et al.A large-scale multicenter study of long-term outcomes after endoscopic resection for submucosal invasive colorectal cancer. Endoscopy. 2013;45:718–724. - PubMed
LinkOut - more resources
Full Text Sources