

Virological Failure and Acquired Genotypic Resistance Associated With Contemporary Antiretroviral Treatment Regimens
- PMID: 32904894
- PMCID: PMC7462367
- DOI: 10.1093/ofid/ofaa316
Virological Failure and Acquired Genotypic Resistance Associated With Contemporary Antiretroviral Treatment Regimens
Abstract
Background: There are few descriptions of virologic failure (VF) and acquired drug resistance (HIVDR) in large cohorts initiating contemporary antiretroviral therapy (ART).
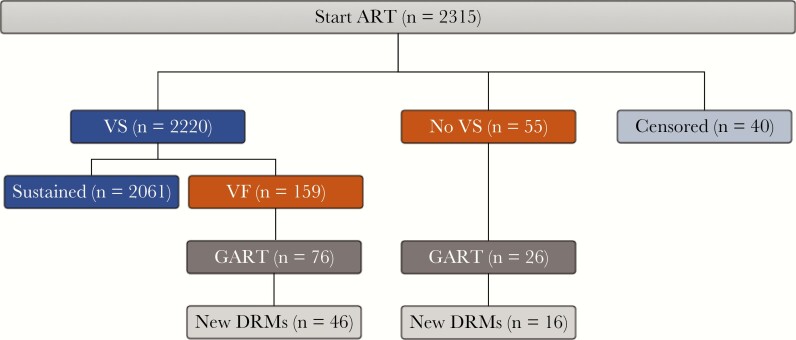
Methods: We studied all persons with HIV (PWH) in a California clinic population initiating ART between 2010 and 2017. VF was defined as not attaining virologic suppression, discontinuing ART, or virologic rebound prompting change in ART.
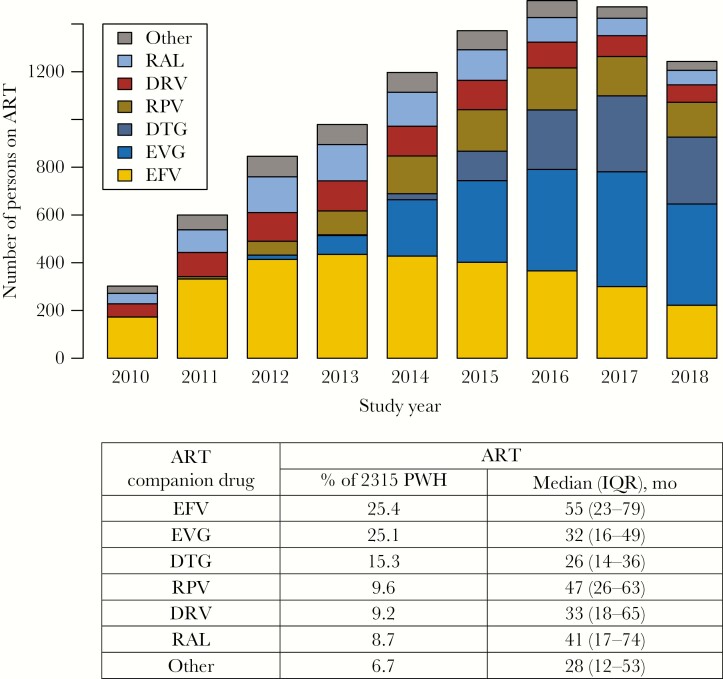
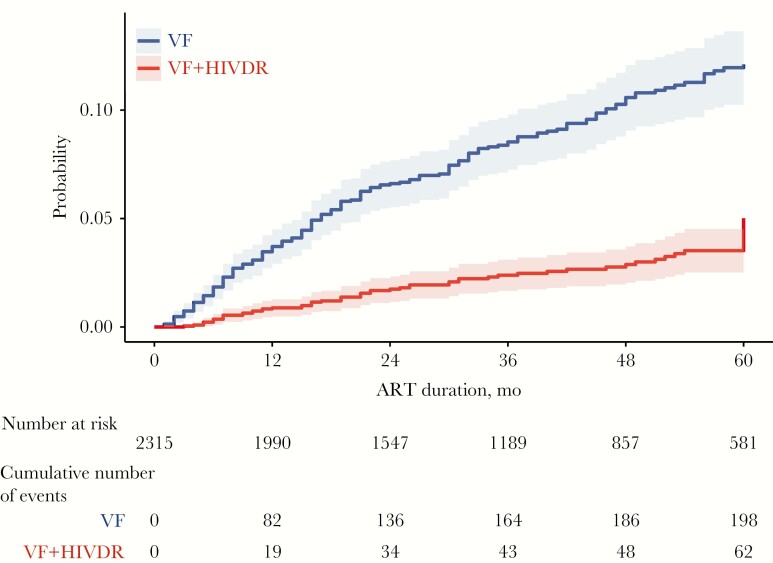
Results: During the study, 2315 PWH began ART. Six companion drugs were used in 93.3% of regimens: efavirenz, elvitegravir/c, dolutegravir, b-darunavir, rilpivirine, and raltegravir. During a median follow-up of 36 months, 214 (9.2%) PWH experienced VF (2.8 per 100 person-years) and 62 (2.7%) experienced HIVDR (0.8 per 100 person-years). In multivariable analyses, younger age, lower CD4 count, higher virus load, and b-atazanavir were associated with increased VF risk; lower CD4 count, higher virus load, and nevirapine were associated with increased HIVDR risk. Compared with efavirenz, dolutegravir, raltegravir, and b-darunavir were associated with reduced HIVDR risk. Risks of VF and HIVDR were not significantly associated with ART initiation year. Of the 62 PWH with HIVDR, 42 received an non-nucleoside RT inhibitor (NNRTI), 15 an integrase-strand transfer inhibitor (INSTI), and 5 a protease inhibitor (PI). Among those with HIVDR on an NNRTI or first-generation INSTI, 59% acquired dual class resistance and 29% developed tenofovir resistance; those receiving a PI or dolutegravir developed just M184V.
Conclusions: Despite the frequent use of contemporary ART regimens, VF and HIVDR continue to occur. Further efforts are required to improve long-term ART virological responses to prevent the consequences of ongoing HIV-1 replication including virus transmission and HIVDR.
Keywords: HIV-1; antiretroviral therapy; drug resistance; virological outcome.
© The Author(s) 2020. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Carr A, Richardson R, Liu Z. Success and failure of initial antiretroviral therapy in adults: an updated systematic review. AIDS 2019; 33:443–53. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
