

The impact of obesity on severe disease and mortality in people with SARS-CoV-2: A systematic review and meta-analysis
- PMID: 32904932
- PMCID: PMC7460942
- DOI: 10.1002/edm2.176
The impact of obesity on severe disease and mortality in people with SARS-CoV-2: A systematic review and meta-analysis
Abstract
Background: Obesity accompanied by excess ectopic fat storage has been postulated as a risk factor for severe disease in people with SARS-CoV-2 through the stimulation of inflammation, functional immunologic deficit and a pro-thrombotic disseminated intravascular coagulation with associated high rates of venous thromboembolism.
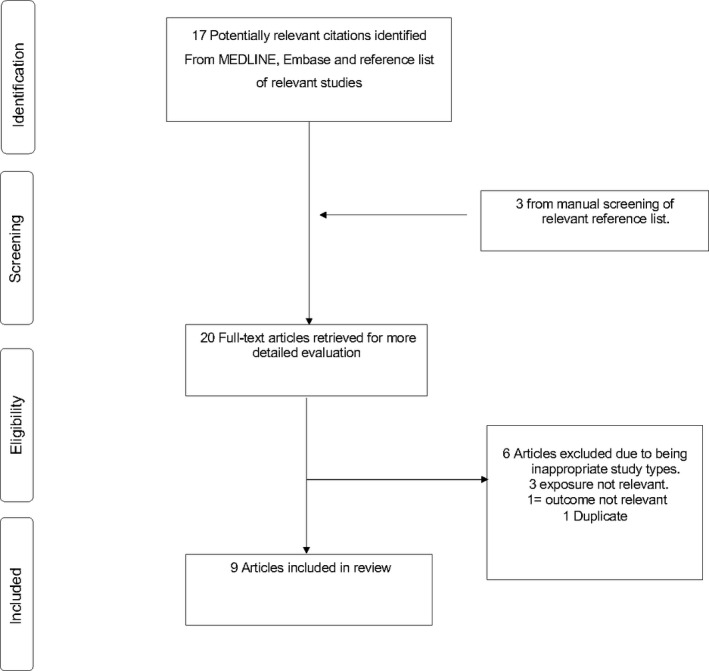
Methods: Observational studies in COVID-19 patients reporting data on raised body mass index at admission and associated clinical outcomes were identified from MEDLINE, Embase, Web of Science and the Cochrane Library up to 16 May 2020. Mean differences and relative risks (RR) with 95% confidence intervals (CIs) were aggregated using random effects models.
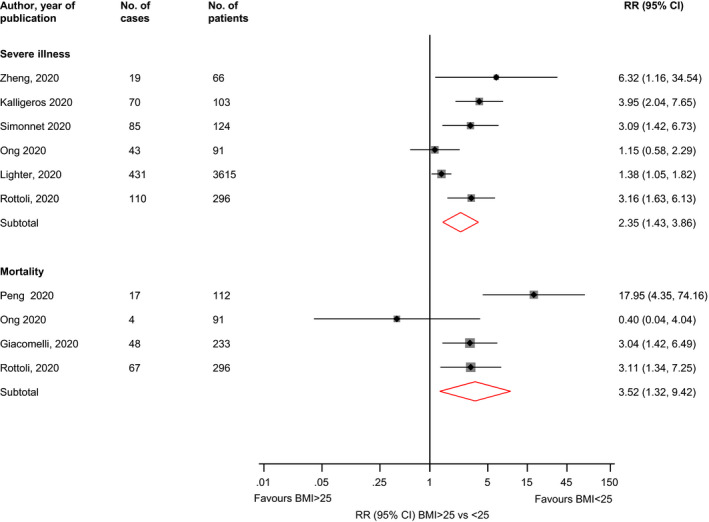
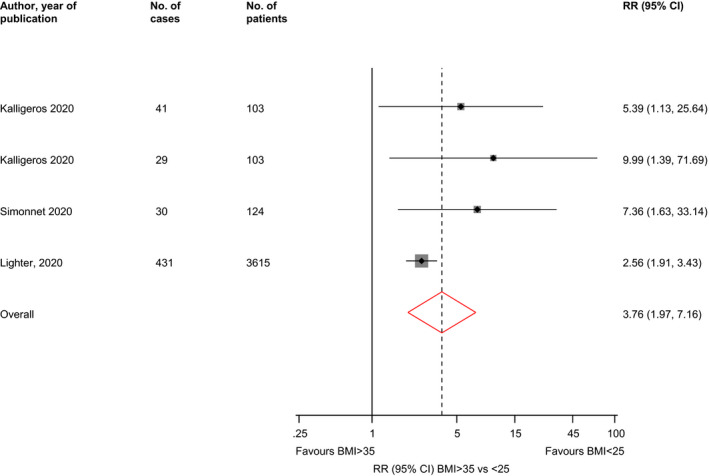
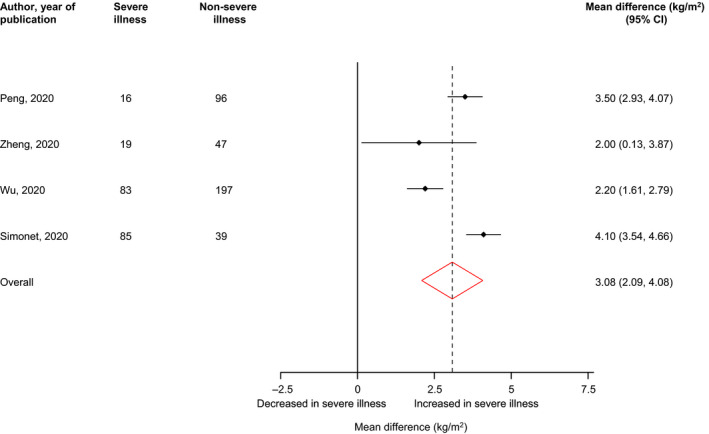
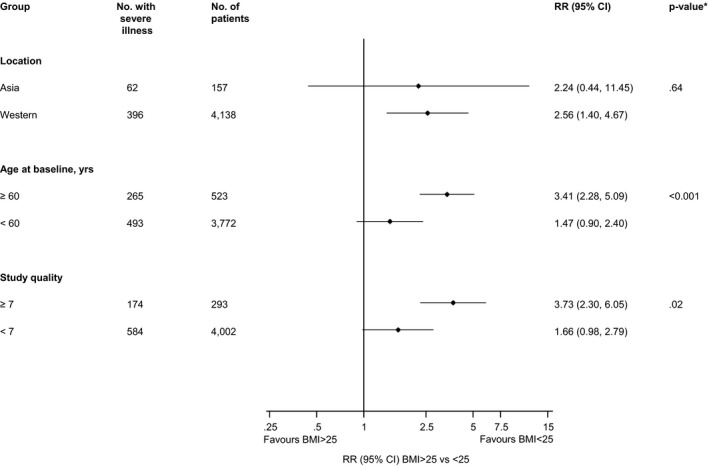
Results: Eight retrospective cohort studies and one cohort prospective cohort study with data on of 4,920 patients with COVID-19 were eligible. Comparing BMI ≥ 25 vs <25 kg/m2, the RRs (95% CIs) of severe illness and mortality were 2.35 (1.43-3.86) and 3.52 (1.32-9.42), respectively. In a pooled analysis of three studies, the RR (95% CI) of severe illness comparing BMI > 35 vs <25 kg/m2 was 7.04 (2.72-18.20). High levels of statistical heterogeneity were partly explained by age; BMI ≥ 25 kg/m2 was associated with an increased risk of severe illness in older age groups (≥60 years), whereas the association was weaker in younger age groups (<60 years).
Conclusions: Excess adiposity is a risk factor for severe disease and mortality in people with SARS-CoV-2 infection. This was particularly pronounced in people 60 and older. The increased risk of worse outcomes from SARS-CoV-2 infection in people with excess adiposity should be taken into account when considering individual and population risks and when deciding on which groups to target for public health messaging on prevention and detection measures. Systematic review registration: PROSPERO 2020: CRD42020179783.
Keywords: SARS‐CoV‐2; mortality; obesity; severe disease.
© 2020 The Authors. Endocrinology, Diabetes & Metabolism published by John Wiley & Sons Ltd.
Conflict of interest statement
KK reports personal fees from Berlin‐Chemie AG/ Menarini Group, personal fees from Sanofi‐Aventis, personal fees from Servier, personal fees from Boehringer Ingelheim, grants from Pfizer, grants from Boehringer Ingelheim, grants from AstraZeneca, grants from Novartis, grants from Novo Nordisk, grants from Sanofi‐Aventis, grants from Lilly, grants from Merck Sharp & Dohme, grants from Servier, outside the submitted work. SS reports personal fees from Amgen, personal fees from Astrazeneca, personal fees from NAPP, personal fees from Lilly, personal fees from Merck Sharp & Dohme, personal fees from Novartis, personal fees from Novo Nordisk, personal fees from Roche, personal fees from Sanofi‐Aventis, personal fees from Boehringer Ingelheim, grants from AstraZeneca, grants from Sanofi‐Aventis, grants from Servier, grants from Janssen, outside the submitted work. MJD reports personal fees and grants from Boehringer Ingelheim, Janssen, Novo Nordisk and Sanofi, and personal fees from AstraZeneca, Eli Lilly, Gilead Sciences Ltd., Intarcia/Servier, Merck Sharp & Dohme, Mitsubishi Tanabe Pharma Corporation and Takeda Pharmaceuticals International Inc.
Figures
Comment in
-
Confluence of obesity and MAFLD during Covid-19 pandemic in a developing country.Endocrinol Diabetes Metab. 2021 Apr;4(2):e00189. doi: 10.1002/edm2.189. Epub 2020 Oct 21. Endocrinol Diabetes Metab. 2021. PMID: 33173833 Free PMC article.
References
-
- Coronavirus Disease (COVID‐19) Pandemic. Geneva: World Health Organisation; 2020.
-
- Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospitalization and critical illness among 4,103 patients with COVID‐19 disease in New York City. medRxiv. 2020.
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
