

Anemia and iron deficiency among chronic kidney disease Stages 3-5ND patients in the Chronic Kidney Disease Outcomes and Practice Patterns Study: often unmeasured, variably treated
- PMID: 32905241
- PMCID: PMC7467578
- DOI: 10.1093/ckj/sfz091
Anemia and iron deficiency among chronic kidney disease Stages 3-5ND patients in the Chronic Kidney Disease Outcomes and Practice Patterns Study: often unmeasured, variably treated
Abstract
Background: International variation in anemia assessment and management practices in chronic kidney disease (CKD) is poorly understood.
Methods: We performed a cross-sectional analysis of anemia laboratory monitoring, prevalence and management in the prospective Chronic Kidney Disease Outcomes and Practice Patterns Study (CKDopps). A total of 6766 participants with CKD Stages 3a-5ND from nephrology clinics in Brazil, France, Germany and the USA were included.
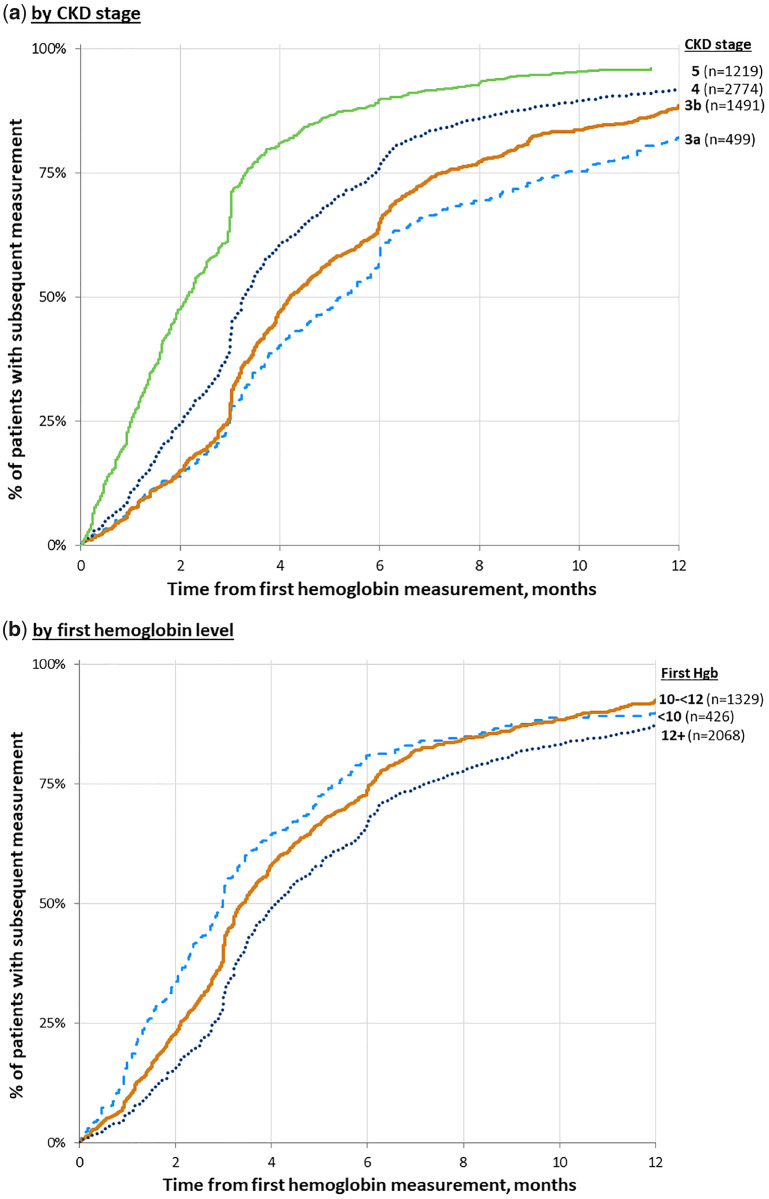
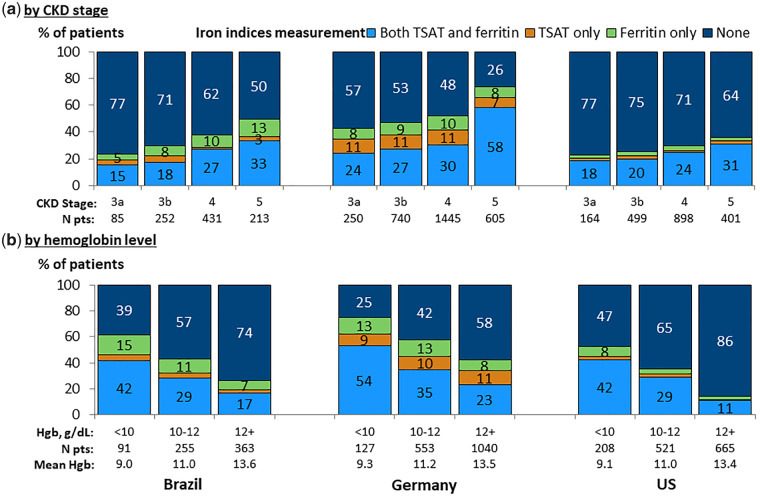
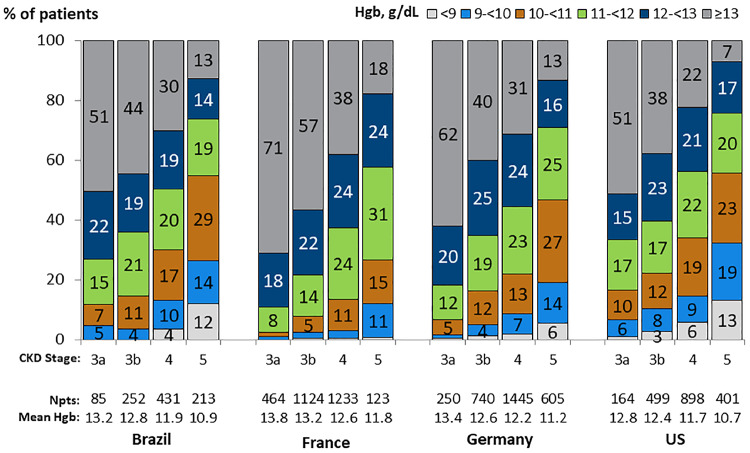
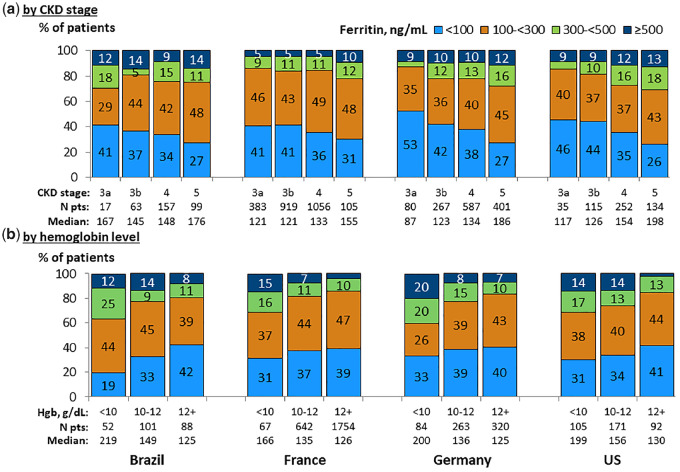
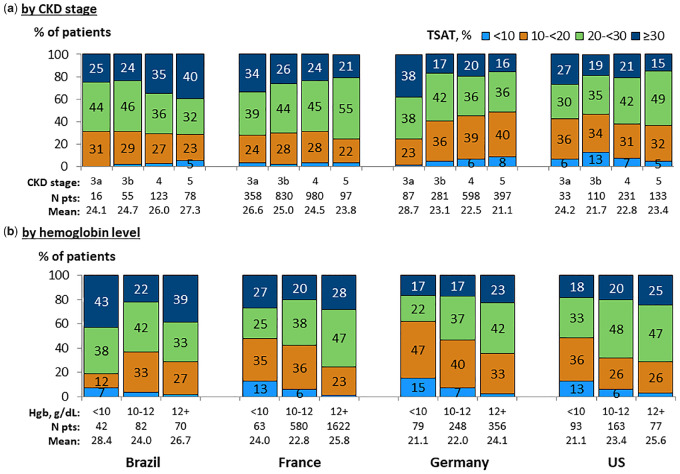
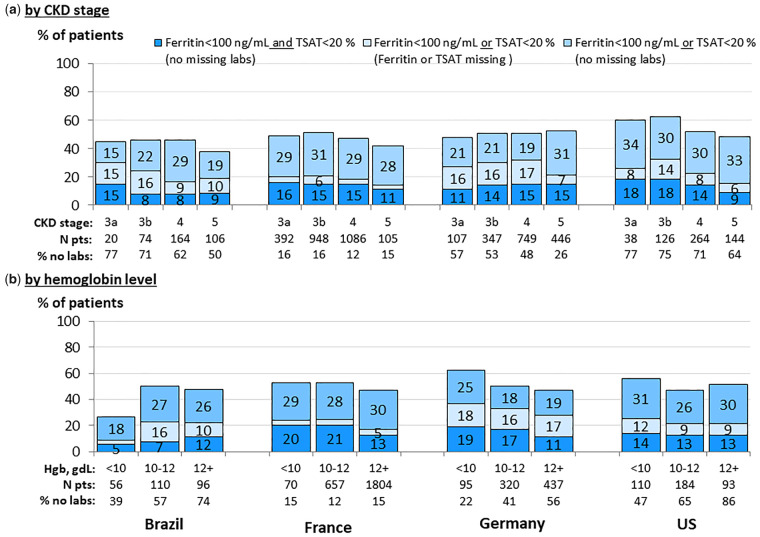
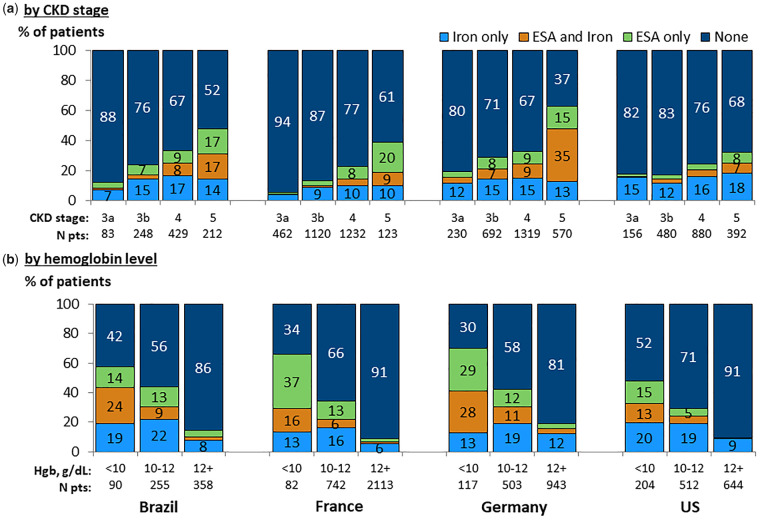
Results: Among patients with anemia (hemoglobin <12 g/dL), 36-58% in Brazil, the USA and Germany had repeat hemoglobin measured and 40-61% had iron indices measured within 3 months of the index hemoglobin measurement. Anemia was more common in the USA and Brazil than in France and Germany across CKD stages. Higher ferritin and lower iron saturation (TSAT) levels were observed with lower hemoglobin levels, and higher ferritin with more advanced CKD. The proportion of anemic patients with ferritin <100 ng/mL or TSAT <20% ranged from 42% in Brazil to 53% in France and Germany, and of these patients, over 40% in Brazil, Germany and the USA, compared with 27% in France, were treated with oral or intravenous iron within 3 months after hemoglobin measurement. The proportion of patients with hemoglobin <10 g/dL treated with erythropoiesis-stimulating agents ranged from 28% in the USA to 57% in Germany.
Conclusions: Hemoglobin and iron stores are measured less frequently than per guidelines. Among all regions, there was a substantial proportion of anemic patients with iron deficiency who were not treated with iron, highlighting an area for practice improvement in CKD care.
Keywords: anemia; chronic kidney disease; erythropoiesis-stimulating agents; iron deficiency; iron supplementation.
© The Author(s) 2019. Published by Oxford University Press on behalf of ERA-EDTA.
Figures
References
-
- Astor BC, Muntner P, Levin A. et al. Association of kidney function with anemia: the Third National Health and Nutrition Examination Survey (1988-1994). Arch Intern Med 2002; 162: 1401–1408 - PubMed
-
- McClellan W, Aronoff SL, Bolton WK. et al. The prevalence of anemia in patients with chronic kidney disease. Curr Med Res Opin 2004; 20:1501–1510 - PubMed
-
- Astor BC, Coresh J, Heiss G. et al. Kidney function and anemia as risk factors for coronary heart disease and mortality: the Atherosclerosis Risk in Communities (ARIC) Study. Am Heart J 2006; 151: 492–50 - PubMed
LinkOut - more resources
Full Text Sources
